Why do cysts form?
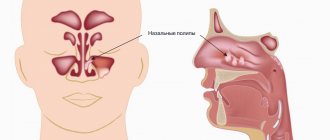
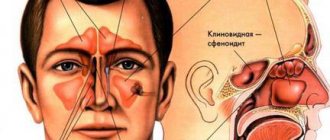
There are 7 sinuses in the facial part of the skull: 3 paired and 1 unpaired. The paired ones are the frontal, maxillary (or maxillary) sinuses and the ethmoidal labyrinths (consisting of several fused cells of the ethmoid bone). Unpaired - wedge-shaped in the body of the bone of the same name. The paranasal sinuses are connected to the nose by narrow canals or anastomoses. Thanks to them, the facial part of the skull is filled with air. The sinuses are located inside the cranial bones, their size is constant. The inside of the sinus cavities are lined with ciliated epithelium or special cells - cilia. These cells are covered with mucus, which flows down with constant rhythmic movements of the epithelial “cilia” into the nose, carrying with it particles of airborne dust.
At CELT you can consult an otorhinolaryngologist.
- Initial consultation – 3,000
- Repeated consultation – 2,000
Make an appointment
Each gland that produces mucus ends in an excretory duct. Sometimes - most often during the process of inflammation - the duct closes, and the gland continues to work for some time. The mucus accumulates, the tissues move apart - this is how cysts are formed, enclosed in a membrane. Such cysts are called true or mucoceles. There are other types of cysts:
- congenital (developmental defects) - often are incidental findings during studies for another reason;
- false - without a membrane, formed in the thickness of the mucous membrane, can empty themselves, develop with chronic runny nose or allergies;
- cavities located at the roots of the teeth of the upper jaw (odontogenic cysts), formed as a result of treatment errors or in the place of underdeveloped tooth germs.
Odontogenic cysts rarely occur on healthy soil. Typically, people who experience this complication have a congenital defect - a low bottom of the maxillary sinus. Sometimes the filling material comes out of the nerve canal, which can cause inflammation and cyst formation.
Mucocele in the maxillary sinus
According to the pathogenetic classification, all cystic lesions of the paranasal sinuses can be divided into three forms: retention cysts, meningocele and mucocele. Retention cysts are the most common form, the localization of which is usually strictly limited. Meningocele is a hernial protrusion of the meninges that occurs due to the pathological development of the fetal skull. Mucocele is a benign, expansive cyst-like formation filled with mucus and lined with respiratory epithelium of the paranasal sinuses. Mucocele grows slowly and is locally aggressive.
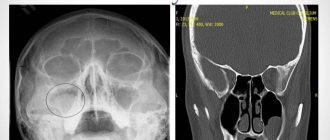
Photo 1. Orthopantomogram
It is believed that a mucocele may cause obstruction of the opening connecting the sinus to the nasal cavity, which leads to the accumulation of fluid. Gradually, producing mucus, the mucocele increases in size and deforms the surrounding bone. The most common causes of mucoceles are chronic infections, allergic diseases, trauma and previous surgical interventions, while the causes of some remain unknown.
Figure 2: CT scan showing a mass in the left maxillary sinus.
Figure 3. Axial view of MRI showing a mass in the left maxillary sinus.
Most mucoceles are localized in the frontal sinus (60%), followed by the ethmoid sinus (30%) and maxillary sinus (10%). Location in the sphenoid sinus is considered very rare. Despite the fact that this formation is benign, a mucocele in the maxillary sinus can grow to large sizes and cause bone destruction. The symptoms manifested are mainly associated with compression of surrounding tissues. The addition of a secondary infection can lead to aggravation of the condition and cause complications, especially in the orbital area.
Photo 4. Aspiration fluid
CT is the principal diagnostic method. CT and MRI images allow the specialist to accurately assess the location of the formation. The traditional method of treatment is excision or enucleation using endoscopic intranasal access.
The purpose of this report is to demonstrate a large mucocele of the maxillary sinus, which is considered rare in patients without previous ENT pathologies. The cyst was enucleated using the Caldwell-Luc method.
Description of a clinical case.
A 39-year-old man with a large mass in the left maxillary sinus, asymptomatic, was referred to the Department of Maxillofacial Surgery. The formation was discovered during an X-ray examination. The patient denies any history of trauma, allergic diseases, or interventions on the paranasal sinuses. The patient has an unremarkable medical history, does not take medications, and is a smoker.
Examination of the oral cavity was unremarkable, with the exception of palpable swelling along the buccal sulcus. X-ray and CT scan showed a homogeneous mass filling the left maxillary sinus (Figures 1,2). Approximate size 5x5 cm.
A puncture of the formation was performed under local anesthesia. A light yellowish fluid was aspirated from the mass. After this, the Caldwell-Luke operation was performed, the left maxillary sinus was cleaned and examined (Photo 4,5). Histopathological examination identified the mass as a mucocele. The recovery process was uneventful in a short period. The patient is under the supervision of specialists.
Photo 5. During surgery
Discussion.
The term mucocele was introduced by Rollet in 1896, and the first histological description was made by Onodi in 1901. The most common location of mucocele is in the frontal sinus, somewhat less commonly in the ethmoid and sphenoid. In the maxillary sinus, mucocele also occurs very rarely, about 10% of cases. The symptoms manifested are mainly associated with compression of surrounding tissues. Mucoceles of the frontal and ethmoid sinuses are often associated with headaches and sometimes blurred vision. A mass in the maxillary sinus usually causes symptoms of obstruction and visual defect. Mucoceles are considered benign formations, however, they can have a detrimental effect on the surrounding vital structures of the orbit and skull. In addition, conditions such as sinusitis, nasal congestion and anosmia appear. Although the patient in question had a large mucocele, he was completely asymptomatic.
Differential diagnosis presents certain difficulties. In the absence of bone erosion, mucoceles are distinguished from retention cysts, sinusitis and polyposis of the paranasal sinuses. In cases where bone damage is extensive, it should be differentiated from malignant conditions: spinocellular carcinoma, cystadenocarcinoma, plasmacytoma, melanocarcinoma, schwannoma and tumors of odontogenic origin.
CT scans in axial and direct projections are the optimal method for detecting mucoceles. The sinus is usually darkened, dilated and with damage to the bone walls. The sinus cavity is filled with fluid and soft tissue. It is preferable to perform CT images; MRI can be useful in controversial conditions to determine fluid or tissue in the lumen. In our case, CT showed a homogeneous formation completely filling the maxillary sinus.
Treatment traditionally consists of enucleation or enucleation of the cyst through an external approach. However, Blackwell in 1993 described a successful intervention using an endoscopic technique for antrostomy of the maxilla. Since then, endoscopic techniques have been increasingly developed, and a method of access through the lower nasal meatus has now been described. After surgery, the sinus configuration may remain unchanged, improve slightly, or return to normal. Nkenke suggests evaluating results at least 2 months after the intervention, as he considers this period necessary for recovery. External access involves tissue dissection, sinusotomy and mucocele removal. In our case, the Caldwell-Luc method was used under local anesthesia.
Conclusion.
Mucoceles in the maxillary sinus are considered rare. The present case describes a large mucocele in the maxillary sinus of a patient who had no history of any complaints or problems with ENT organs. The treatment was surgical, Caldwell-Luc surgery. Recovery was uneventful with a short follow-up period.
Authors:
Fidevs Akpek, Researcher, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Abant Izzet Baysal University, Bolu, Turkey
Ismail Akkas, Assistant Professor, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Abant Izzet Baysal University, Bolu, Turkey
Orcum TOPTAS, Assistant Professor, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Abant Izzet Baysal University, Bolu, Turkey
Fatih Ozan, Associate Professor, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Abant Izzet Baysal University, Bolu, Turkey
Signs
Quite often, cysts of the paranasal sinuses do not manifest themselves for a very long time, until they reach gigantic sizes, occupying all the free space. A person may be bothered by:
- headache for no apparent reason, has no pattern and cannot be treated with painkillers;
- a feeling of pressure on the eyes, strange discomfort in the upper jaw;
- an unpleasant feeling of mucus running down the throat (mucus flows down the back of the throat);
- smell disorders - occur with a cyst of the sphenoid sinus,
- the release of a clear, light-colored liquid without any admixture of pus or blood during spontaneous rupture and emptying of the cyst.
When a cyst occurs, the emptying of the sinuses may be disrupted, reducing their natural cleansing ability. Then inflammation occurs, which is manifested by constant nasal discharge, increased headaches, the appearance of an unpleasant odor, increased body temperature, and the development of chronic sinusitis.
In the presence of a cyst, allergic manifestations are more severe, losing their seasonality and turning into a permanent problem.
Nasal breathing is rarely difficult, only when the cyst enters the nasal cavity or is inflamed.
Computed tomography of the sinuses
- Cost: 5,000 rub.
More details
Odontogenic cysts have unpleasant manifestations. There is lacrimation, swelling, and acute pain similar to neuralgia. If the cyst suppurates, signs of general intoxication appear: fever, severe headache, nausea or vomiting, loss of appetite, weakness.
2. Reasons
The immediate cause of muco/pyocele is mechanical bursting pressure on the walls of the frontal sinus from the inside, from accumulated mucous or purulent masses. If this situation continues long enough, the bone walls begin to thin and become deformed in the direction of stretching.
In turn, a complete or partial blockage (obstruction, obliteration, obstruction) of the canal connecting the sinus with the nasopharyngeal cavity leads to the accumulation of contents. This is facilitated by fibrosing processes - tissue degeneration, stenosis and the formation of adhesions during chronic inflammation, scarring after injuries, etc. Less commonly, the cause is polyposis, a tumor, or severe curvature of the nasal septum.
Infection, if it occurs, is caused by the same mechanisms that lead to the development of frontal sinusitis: the spread of infection from the affected nasopharynx, neighboring sinuses, other adjacent structures, or the penetration of a pathogen through the blood or lymph.
Visit our Otolaryngology (ENT) page
Diagnosis of a cyst
A simple examination cannot detect a cyst. Based on a combination of complaints and other data, an ENT doctor may suspect that a person has a cyst in the paranasal sinuses. To clarify the diagnosis, instrumental diagnostics are needed, which allows one to identify the cyst.
The first step is an x-ray or computed tomography, which allows you to determine the relative position of the bones of the skull and nasal sinuses, their size and structure. Computed tomography provides a 3-dimensional image.
In unclear cases, especially during initial treatment, probing or puncture of the maxillary sinuses is performed. The goal is to obtain the contents and examine them in a laboratory setting. The punctate examines the presence of cells and their characteristics, the biochemical composition of the liquid, and the presence of bacteria.
After all the research has been carried out and the diagnosis has been clarified, treatment must be started.
3. Symptoms and diagnosis
Between the actual onset of bone deformation and the appearance of tangible manifest symptoms, it can take from a year to 5-6 years or more.
As a rule, the patient pays attention to frequent headaches of a pulling, dull, aching nature, localized in the frontal lobes, less often radiating to the bridge of the nose or temples. Then periorbital pain occurs, deformation of facial proportions becomes noticeable, and a gradually growing bulge appears in the corner of the eye. Palpation examination of this protrusion is usually accompanied by crepitus (dry rustling, parchment crunch). With further progression, exophthalmos is formed, the eyeball also moves downward, visual disturbances appear and increase, which, in the absence of adequate help at this stage, can result in severe complications up to atrophy of the optic nerve head, retinal detachment and loss of vision in the affected eye.
Further accumulation of contents in the muco(pio)cele can lead to the formation of a fistula and the spread of the infectious and inflammatory process to adjacent cavities and structures. The consequences of this can be the most severe - meningoencephalitis, panophthalmitis, periorbital cellulitis (orbital cellulitis), etc.
When contacting in the early stages, such mandatory diagnostic procedures as analysis of complaints, careful history taking and standard examination of ENT organs (rhinoscopy, otoscopy, etc.) may not be enough. Of the instrumental studies, the most informative are radiography, ultrasound, tomography (CT or MRI); Sometimes probing or puncture of the frontal sinus is indicated.
Consultation and examination with related specialists is almost always necessary - first of all, with an ophthalmologist, and also, if indicated, with a neurologist, oncologist, etc.
About our clinic Chistye Prudy metro station Medintercom page!
Treatment methods for sinus cysts
Treatment for cysts is not always surgical. Conservative methods are effective for small cysts. Surgery can be started only after acute inflammation has resolved. Therefore, the ENT doctor first prescribes conservative treatment. Whether surgery is necessary or not is decided solely by the attending ENT doctor. In some cases, a fairly long-term observation of the growth of the cyst and its “behavior” is required, which reveals all the nuances of formation in a particular person.
The patency of all anastomoses through which the sinuses communicate with the nose requires attention. Odontogenic cysts require the participation of a dentist; without him, treatment is not carried out.
Endonasal maxillary sinusotomy
- Cost: 40,000 - 75,000 rubles.
- Duration: 20-40 minutes
- Hospitalization: 1-2 days in hospital
More details
Surgical removal of paranasal sinus cysts is performed at CELT using the endoscopic method, which is the most gentle method. A small probe with a video camera and special instruments is used. The instrument is inserted into the nose - after anesthesia, of course. No incisions are made on the face or anywhere else. Thanks to a video camera, the surgeon sees everything that is happening on a large screen, where all the details are clearly visible. The cyst is first emptied, then its membrane, if any, is removed.
If the contents are purulent, additional rinsing with antibiotics is performed. The final stage of the operation is the formation of a full-fledged anastomosis between the sinus and nose, which prevents relapses. Of course, in the postoperative period, supervision by an ENT doctor is required.
It is also important to examine and treat children and adolescents. Often cysts first appear between the ages of 10 and 13 years, when they form on tooth germs that are displaced from their physiological place or impacted. Baby teeth can also become inflamed and give rise to the formation of a cyst. Treatment of children is carried out in a day surgical hospital for maximum comfort.
The CELT Clinic has accumulated a wealth of experience in the treatment of ENT pathologies, including cysts. By contacting otolaryngologists at CELT, you can be confident in a competent examination and treatment by experienced specialists.
4.Treatment
It is easy to see that there are no conservative methods for eliminating muco/pyocele of the frontal sinus. Even forced complete drainage of the sinus does not reconstruct the normal anatomy of the bony cranial structures. Therefore, in all cases, the question is raised about frontotomy (opening the frontal sinus) with evacuation of the contents, sanitation of the surgical field, restoration of normal sinus ventilation and, if indicated, plastic surgery. The operation is performed under powerful antibiotic, anti-inflammatory and decongestant cover, drainage is left until the surgical wound is completely healed and scarred.
The prognosis is favorable in the absence of serious complications (see above), which require the use of separate, sometimes emergency care protocols.
Our services in otorhinolaryngology
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| X-ray of the paranasal sinuses | 2 200 |
| MSCT of the paranasal sinuses | 5 000 |
| Endonasal maxillary sinusotomy | 40 000 — 75 000 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions