Maxillary sinus surgery is a surgical treatment of the maxillary sinus.
Author:
- Oganesyan Tigran Sergeevich
ENT pathology expert
5.00 (Votes: 2)
Chronic sinus diseases are widespread. Of these, the most common is chronic inflammation of the maxillary sinus - sinusitis.
When the disease lasts for a long time - for years, the effectiveness of conservative treatment (punctures, nasal lavage and even antibacterial therapy) becomes less and less effective, and the number of exacerbations increases. The presence of a chronic focus of purulent infection in the upper respiratory tract can provoke complications. Along with exacerbations of sinusitis, a person begins to suffer from bronchitis, tracheitis and even pneumonia. This is called "descending" complications - when the infection spreads to the lower respiratory tract. A general decrease in immunity also plays a major role in this, since any chronic infection forces the immune system to work in an enhanced mode, and frequent antibacterial therapy leads to an increase in forms of bacteria with resistance to drugs. In such cases, when all means have been tried, but it is not possible to eliminate the disease or even reduce its symptoms, surgical treatment is indicated - maxillary sinusotomy .
The goal of the operation is to completely remove all affected tissue from the sinus. Since with chronic inflammation the mucous membrane inside the sinus grows rapidly and exceeds the thickness of healthy tissue several times, cysts and polyps can form. An important point of the operation is the revision of the sinus anastomosis. Normally, the maxillary sinus communicates with the nasal cavity through an opening (ostium), which opens into the middle nasal passage. If it works correctly, i.e. is passable for air flow, then when breathing, oxygen enters the sinuses and maintains there an optimal environment for the functioning of the mucosal epithelium and prevents the proliferation of bacteria. Chronically inflamed mucosa can close the anastomosis, thereby maintaining an infection in the sinus cavity. Another reason for the narrowing of the anastomosis can be anatomical features - curvature of the nasal septum, narrowing of the middle nasal meatus due to congenital or acquired enlargement of its structures, for example, the middle concha or the uncinate process.
Indications for maxillary sinusotomy:
- parietal hyperplastic form of sinusitis;
- polyposis-purulent form of sinusitis;
- irreversible changes in the sinus, up to destruction of the bone wall;
- a foreign body in the sinus (for example, filling material that enters the sinus during dental treatment);
- frequent exacerbations of chronic sinusitis (more than 2-3 times a year);
- fungal body in the sinus (occurs as a complication due to long-term antibacterial therapy or the presence of a foreign body).
Why does inflammation develop in the sinus?
Predispose to the development of sinusitis:
- anatomical features (narrowness of the nasal passages, curvature of the septum, narrowing of the sinus mouth, bone defects of the facial skull);
- decreased local and general immunity;
- dental pathology (caries of deep-lying upper molars, radicular cysts), in this case they speak of the odontogenic nature of the process;
- a chronic source of infection in the ENT organs, which creates conditions for the activation of opportunistic flora;
- allergic background (hay fever, allergic rhinitis, etc.);
- various neoplasms in the nose and paranasal sinuses that interfere with sinus ventilation.
Inflammation of the paranasal sinuses is usually infectious in nature. Moreover, in the acute form of the disease, we are talking about the penetration of pathogenic viruses or bacteria from the outside, which leads to swelling in the nose and paranasal sinuses. But the main cause of chronic sinusitis is the activation of one’s own opportunistic flora under conditions of prolonged stagnation of mucus.
Methods of maxillary sinusotomy
1. Radical surgery on the maxillary sinus according to Caldwell-Luc.
The surgical technique was developed and used by GW Caldwell and N. Luc at the beginning of the last century. To access the sinus, an incision is made under the upper lip, then a fragment of bone is removed from approximately the second to the fifth tooth, resulting in a fairly large entrance to the sinus. This, on the one hand, allows you to freely examine and remove pathologically altered tissues, on the other hand, such an intervention is traumatic - the wound takes a long time to heal, the anterior wall of the sinus remains without a bone wall and the symptoms of inflammation may resume, since the operation does not restore the natural drainage of the sinus. This technique is not currently used.
2. Microsinusrotomy.
A modern and gentle version of the operation. Access to the sinus is also through the front wall (under the upper lip). The hole is formed with a small diameter - about 5-7 mm. A trocar is used for this. This is a funnel with a sharp base that passes through the mucous and bony walls, forming a neat and smooth entrance into the sinus through which an endoscopic camera can be inserted to examine the cavity and endoscopic instruments for removal. This operation is less traumatic due to the ability to use an endoscopic instrument. Therefore, the postoperative period is easy - the patient does not feel pain or discomfort, and the wound heals quickly.
Microsinusrotomy is often performed to remove local sinus formations - cysts, foreign bodies, i.e. when the anastomosis functions well enough and does not need to be expanded.
3. Endoscopic maxillary sinusotomy with access through the nasal cavity.
This operation is indicated for chronic purulent or hyperplastic sinusitis, when the sinus mucosa is changed throughout its entire length. Such conditions are often the result of improper functioning of the sinus anastomosis, to the point that it can be completely blocked. Access to the sinus can be gained through the middle or lower nasal passages, which are located on the lateral (outer side) wall of the nose. Inspection and expansion of the anastomosis is possible only with access through the middle nasal meatus; such an operation will be the most functional and effective. It is worth noting that endoscopic operations require highly qualified operating otolaryngologist and knowledge of the endoscopic anatomy of the nose. At the moment, such operations are the most advanced and modern.
| Methods of maxillary sinusotomy | Complications |
| Radical surgery on the maxillary sinus according to Caldwell-Luc | Damage to the second branch of the trigeminal nerve with subsequent neuropathy |
| Microsinusrotomy | |
| Endoscopic maxillary sinusotomy with access through the nasal cavity | Postoperative bleeding |
Main symptoms
The most common signs of damage to the maxillary sinuses include:
- Mucopurulent discharge from the nose. They are usually one-sided and intensify with exacerbation of the process and change in head position.
- Pain under the eye and near the wing of the nose, a feeling of heaviness and pressure in the depths of this area.
- Difficulty in nasal breathing, persistent runny nose.
- Headache.
- General signs of intoxication (fever, weakness, decreased performance, etc.).
Over time, almost the entire system of the paranasal sinuses can be involved in the inflammatory process, which further worsens the patient’s well-being.
Long-term inflammation also negatively affects the functioning of the immune system, reduces the adaptive abilities of the entire body, and increases the risk of local and systemic complications. Therefore, it is necessary to strive to completely cure chronic sinusitis.
Maxillary sinusotomy: how and where it is performed
See also Treatment of ENT diseases Sinusitis Treatment of chronic sinusitis Sinusitis in a child
Sinusotomy is the most effective operation for the treatment of chronic sinusitis. It can be performed using classical surgical instruments, but currently preference is given to minimally invasive endoscopic techniques.
The use of an endoscope allows you to visually control all manipulations, increases the accuracy of the procedure, and significantly reduces its trauma and the level of blood loss. Recovery after endoscopic maxillary sinus surgery is faster and easier than after classical sinus surgery. Patients do not require prolonged hospitalization and can leave the clinic after 2–3 hours.
In the specialized ENT Clinic of Dr. Korenchenko, endoscopy is a key therapeutic and diagnostic procedure. This practice increases the information content of the examination of each patient, minimizes the traumatic nature of manipulations, and increases the effectiveness of treatment even for chronic and complicated forms of sinusitis.
How to treat perforation of the maxillary sinus floor?
A decisive preventive action that will prevent the inflammatory process of the maxillary sinus when an anastomosis has formed is the immediate closure of the communication. Closing the anastomosis with the maxillary sinus is performed using a trapezoid-shaped mucoperiosteal section formed at the beginning of the oral cavity, so that it is possible to peel off the flap a few millimeters above the transitional fold.
Before laying the mucoperiosteal area, the sharp edges of the alveolar process are smoothed with a special tool, parts of the flap and soft tissues from the side of the palate are cut to a width of 1-2 mm for better connection and better conditions for healing by primary intention. Before starting the procedure, the wound is treated with penicillin or streptomycin.
To ensure the safety of the flap, it is necessary to cover it and the adjacent tissue with gauze and a protective plate.
If a maxillary sinus anastomosis occurs during removal of the apical part of the root, removal of wisdom teeth, or during surgery for jaw cysts, it is necessary to suture the wound.
In case of perforation of the maxillary sinus during resection of the root apex, removal of wisdom teeth, or during operations on jaw cysts, the wound must be closed using closely spaced sutures.
Endonasal opening of the maxillary sinus using video technology
Endonasal opening of the maxillary sinus is an endoscopic operation in otorhinolaryngology aimed at treating diseases of the maxillary sinuses.
The method is based on surgical expansion of the natural anastomosis or opening the walls of the maxillary sinuses using endoscopic instruments from the side of the nasal cavity. Thus, optimal conditions are created for accurate diagnosis, effective treatment and prevention of a number of pathologies.
The procedure is carried out under endoscopic control and does not leave behind visible scars or scars - all manipulations are carried out in the nasal cavity using microsurgical and endoscopic methods. Radio wave technology is widely used.
Advantages
- an effective method for diagnosing, treating and preventing pathologies of the maxillary sinuses;
- endoscopic maxillary sinusotomy does not require general anesthesia and can be performed on an outpatient basis;
- the procedure eliminates the need for large-scale open surgery on the maxillary sinuses using the traditional method with increased trauma;
- high safety, minimal risk of complications;
- no need for long-term rehabilitation;
- good cosmetic effect, since endoscopic methods do not require skin incisions and trephination of the anterior wall of the maxillary sinus.
Indications
- chronic hypertrophic sinusitis;
- sinus fungus;
- chronic sinusitis that does not respond to conservative therapy;
- cysts and polyps of the maxillary sinuses;
- developmental anomalies that prevent puncture and lavage of the maxillary sinuses;
- benign neoplasms of the maxillary sinuses;
- foreign bodies of the maxillary sinuses;
- lack of effect from conservative therapy.
Contraindications
- allergic reactions to local anesthetics;
- pregnancy;
- acute infectious diseases of the ENT organs;
- bleeding disorders caused by blood disease or medications;
- malignant neoplasms;
- severe diseases of the cardiovascular system, decompensated diabetes mellitus.
Preparation
- general blood test, blood coagulation test (coagulogram), blood sugar test, blood tests for HIV, viral hepatitis B and C, syphilis;
- ECG;
- X-rays of the facial bones or computed tomography may be required.
Procedure
- endoscopic maxillary sinusotomy is performed on an outpatient basis;
- patient position – sitting or reclining on an otorhinolaryngological chair, with support under the head;
- the procedure is carried out under local infiltration and application anesthesia - the nasal mucosa is lubricated with 10%, injected with a 1-2% lidocaine solution;
- in the most common version of endoscopic maxillary sinusotomy, which involves expanding the natural anastomosis of the maxillary sinuses with the nasal cavity, it is necessary to remove the middle turbinate and the uncinate process to gain access to the anastomosis and space for maneuver;
- after removing the middle turbinate, the probe locates the hole through which the maxillary sinus communicates with the nasal cavity - it serves as an anatomical landmark for the surgeon;
- using reverse cutters, a shaver or other instruments, the inner wall of the maxillary sinus is opened, starting from the anastomosis;
- the purpose of the procedure is to obtain a good overview and access to examine the contents of the maxillary sinus using an endoscope;
- if necessary, they switch to working directly in the cavity of the maxillary sinus - excising neoplasms, polyps, removing hypertrophied mucous membrane, foreign bodies, etc. (all removed tissues are sent for histological analysis);
- after completion of the procedure, the maxillary sinus is washed with antiseptic solutions, a hemostatic sponge is installed, or an anterior nasal tamponade is performed;
- it is possible to install drainage in the maxillary sinus;
- The duration of the procedure is 45-60 minutes.
Rehabilitation
- one of the advantages of endoscopic maxillary sinusotomy is the absence of the need for hospitalization and long-term rehabilitation;
- in the first few days the patient may experience pain, swelling of the cheekbones on the operated side, headaches, toothache, and bruising;
- If you have severe pain, you can take a pain reliever recommended by your doctor;
- in order to prevent infectious complications, antibacterial therapy is carried out;
- It is prohibited to smoke, drink alcohol, visit a sauna or bathhouse, blow your nose, or undergo physical activity;
Accurate compliance with the otolaryngologist’s instructions is an important component for a favorable outcome of the operation.
Recovery period
After the operation, the patient is prescribed antibiotics for a period of 5-7 days. It is necessary to regularly rinse the nasal cavity and treat its mucous membrane with recommended medications (drops, sprays). If the operated area is very painful, it is acceptable to take painkillers. You should not blow your nose; wipes are used for nasal hygiene. You need to sneeze carefully so as not to tear the seam.
How long it takes for the operated area to heal depends on the patient’s behavior. The postoperative period involves the following recommendations:
- exclusion of physical activity;
- observation by an ENT doctor;
- refusal to visit the bathhouse, beach, solarium, exposure to the scorching sun, or too high a temperature when washing;
- avoiding hypothermia;
- careful oral hygiene;
- refusal to eat food of extreme temperature, salty, spicy, alcoholic drinks;
- mandatory rinsing with antiseptic solutions after eating;
- prevention of infectious diseases to avoid re-development of sinusitis.
Following these tips will help speed up recovery and avoid possible complications and consequences.
Principles of treatment
Properly selected treatment for sinusitis is aimed at solving several problems:
- Improving the functioning of the sinus anastomosis by reducing swelling of the mucous membrane.
- Decreased volume of mucus secreted.
- Evacuation of pathological contents from the sinus.
- Elimination of the infectious factor.
- Fight inflammation.
In the initial stages, it is often possible to cure sinusitis without surgery, with the help of well-chosen drug therapy, physiotherapy and rinsing. In more advanced cases, the doctor has to resort to surgical methods.
What operations are performed
Surgical treatment for sinusitis may include:
- Puncture or puncture of the sinus for immediate evacuation of the main part of the secretions and administration of the drug. It is performed with a special needle under local anesthesia. It allows you to quickly alleviate the patient’s condition, but does not always lead to a lasting result. Puncture is most often performed for acute inflammation without purulent complications.
- Maxillary sinus, opening the maxillary sinus to gain access to its internal walls. To do this, an incision is made near the upper gum or under the middle or lower turbinate; less commonly, access is used through the facial part of the cheek. Thanks to a maxillary sinus, the doctor is able to completely remove the pus and thoroughly rinse the affected sinus, eliminate neoplasms and granulations (superficial inflammatory growths), and create the drainage necessary for the outflow of secretions.
There are also less popular procedures (for example, balloon sinus repair). They do not always give a lasting effect and quite often lead to relapses, so they are used mainly as an addition to the main operation.
Why CELT?
The CELT Clinic is a multidisciplinary medical institution where you can get advice, diagnostic tests, and treatment from leading domestic specialists. The operation “endoscopic maxillary sinusotomy” is performed by otolaryngologists with extensive experience in research and practical work. By contacting us, you can be sure that the operation will:
- absolutely safe;
- as efficient as possible;
- painless due to the use of effective anesthetics.
We guarantee to minimize the possibility of complications, as well as a minimal recovery period.
Indications and contraindications for surgery
Sinusitis is the most common type of sinusitis. Most often it occurs as a complication of a respiratory infection. Often the cause of sinusitis is pathologies occurring in the periapical tissues of the upper teeth.
Inflammatory diseases in the maxillary cavities are treated in different ways. In the uncomplicated course of such diseases, antibiotics, nasal drops, nasal lavage and physiotherapy are used.
In more severe cases, they resort to puncture of the maxillary sinuses to remove purulent contents and rinse. Sinusotomy is the most radical treatment for sinusitis, used when other methods do not bring results.
Indications for maxillary sinusotomy are the following pathologies:
- chronic sinusitis, if conservative therapy is ineffective;
- purulent sinusitis, occurring in an acute form, with complications (a purulent process is indicated by the appearance of an unpleasant odor from the nose);
- sinusitis of odontogenic etiology (infection penetrates into the sinus of the upper jaw from the roots of the upper teeth);
- tumor processes of various types;
- sinus cysts;
- detection of a foreign body in the maxillary sinus (a tooth fragment, filling material that penetrated into the sinus through a tooth socket, particles of synthetic materials after intraosseous implantations);
- nasal polyps;
- blood clots;
- damaged walls of the maxillary sinuses.
Sometimes surgical interventions on the maxillary sinuses cannot be performed. A relative contraindication is exacerbation of a chronic inflammatory process in the sinuses. It is necessary to first relieve acute symptoms, except in cases where an acute purulent process develops, threatening dangerous complications (the development of meningitis, sepsis, periostitis). Then the operation is undertaken in the acute period to prevent aggravation of the patient’s condition.
Surgery is not performed for the following diseases:
- acute infections, aggravated chronic diseases;
- severe cardiovascular and pulmonary pathologies in the stage of decompensation;
- insufficiency of liver and kidney function;
- decompensated diabetes mellitus;
- diseases accompanied by blood clotting disorders.
Patients carrying a child are recommended to choose gentle methods of maxillary sinusotomy that do not require general anesthesia.
Preparation
Before prescribing a maxillary sinusotomy, the patient is advised to undergo a thorough examination. It includes:
- examinations by a therapist, otolaryngologist, dentist;
- general blood and urine tests;
- coagulogram;
- bacteriological culture of maxillary sinus discharge;
- fluorography;
- ECG;
- radiography of the sinuses;
- CT or MRI of the skull.
Such surgical interventions are usually carried out as planned and are scheduled for the morning. The patient should not eat for 8-12 hours before surgery.
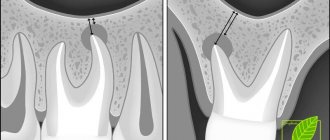
Diagnosis of perforation of the maxillary sinus floor
Checking for perforation of the maxillary sinus floor involves a comprehensive analysis of the typical clinical picture. It is necessary to take into account the condition of the socket of the extracted tooth, the presence of air bubbles, and bleeding from the nasal cavity. An X-ray examination is done, which shows the area of the hole with high accuracy.
The dentist may prescribe a procedure to insert a probe into the perforated canal. This will determine the presence of a bone bottom in the wound. The probe should pass through soft tissues without hindrance, without stopping or clinging to foreign bodies.
X-ray analysis will allow you to see darkening, characteristic of the presence of an accumulation of blood clots. In addition, X-ray images clearly show filling materials, implants, and fragments of tooth roots. Often, radiography uses a bright substance to clearly see the condition of bone and other types of tissue. To do this, the substance is placed into the cavity through the fistula.
An instrumental diagnostic method – computed tomography – will help determine the degree of perforation and the presence of foreign bodies.
If perforation is suspected, general clinical tests are prescribed to help determine the existence of infection in the human body.