A beautiful smile is the dream of every person, and it’s good when it’s natural, but this is becoming less and less common. Under the influence of many negative factors, such as the environment, nutrition, hygiene, injuries, the problem of missing several teeth occurs in many people. Removable dentures come to the rescue. They are attached to existing teeth with clasps. What kind of devices are these, what types are there and what harm can they cause?
Concept and structure of clasps
Clasps are special clamps with which a removable denture is attached to the teeth. In addition, these clamps distribute the chewing load evenly over the entire surface of the jaw.
They consist of the following elements:
- Shoulder. The part that covers the tooth, in turn, is divided into supporting (maintains rigidity and prevents lateral movement) and retaining (provides fixation of the prosthesis).
- Body. The spring base of the clamp, connecting all its fragments and located on the contact surface of the crown.
- Process. Designed for attaching the lock to the prosthesis frame.
The support-retaining fixture also contains an occlusal pad, which allows you to hold the tooth without displacement under the action of angular force. There is also an anchor part with which the clamp is connected to the metal frame.
READ ALSO: how and why are dental veneers used?
Functions assigned to the fixing element
Fixing prosthetic elements must perform 3 functions simultaneously:
- Support. The clasp always rests on the tooth and transfers part of the load to it when chewing.
- Holding/fixing. The overall structure remains motionless and does not fall off during chewing or talking.
- Coverage. If the prosthesis is in the mouth without a fixing device, it will soon move to the side and cease to perform its functions.
Clasps for dentures are an essential part of the structure, without which restoration of chewing function in full is impossible.
Classification: types and features of clasps
Fixators are different depending on the prosthesis, material, and functions performed. The most popular clamps include:
- Bonneville. It consists of two onlays that are fixed in the fissures of molars and premolars. They are used for unilateral missing teeth.
- Jackson. Reversible design, which is a loop. Can be cast or wire.
- Dentoalveolar. Made of plastic, reinforcement possible. It is used when it is necessary to achieve an aesthetic effect.
- Round one-shoulder. They are usually folded onto the molars.
- Schwartz. It bends out of the orthodontic wire and occupies the interdental space. It can be single-link or multi-link.
- Adams. A button lock, consisting of two fixing protrusions, curved towards each other, and two bodies, on the inside turning into processes.
- Duisings. It is bent like a Jackson clasp, but has two semicircular bends at the shoulder, two bodies and two appendages.
- Reichelman. It differs from others in the shape of the lining, which looks like a transverse bar, which goes through the chewing surface into the inside of the oral cavity.
Classification
In dentistry, it is customary to use various criteria to differentiate clasps. So, from the point of view of the materials used for manufacturing, there are:
- Metal models (nickel, chrome-cobalt, precious metals);
- Polymer products;
- Combined options.
Based on the creation method, a distinction is made between stamped and bent-cast structures. At the same time, clasps are also divided into retaining and support-retaining, and from the point of view of shape they are divided into strip, round and semicircular. The connection of the retainer to the base is carried out using a rigid, springy or joint method.
How should the clasps be positioned?
Depending on the desired result, the clamps are located:
- below the equator of the tooth (used more often on retaining dentures),
- above the equator line (in support-holding),
- on the occlusal surface (used in supporting orthodontic structures).
Clasp clamps are positioned for a good fixing effect, taking into account the following factors:
- the object for installation of the fixator must be healthy and motionless, have the correct anatomical shape,
- fixatives should not injure the mucous membrane,
- refurbishment must be carried out
- With multi-link retainers, there must be sufficient space between the teeth.
Boundary line
The choice of clasp for prosthetics directly depends on the position of the boundary line, for which there are five options:
- Location from the contact point in the defect area to the middle part of the proximal surface of the adjacent unit. In such cases, the use of Roach or Bonigrad models is recommended.
- The passage of the equator through the central part of the approximal region, with a smooth rise to the contact point of the adjacent element. Includes installation of an Acker clasp.
- The diagonal position of the equator and the passage of an extended boundary line in the area of the defective chewing surface, with a tangential intersection of the supporting element and ending on the opposite side of the tooth neck. The preferred model is the Ney clasp.
- The high position of the equator, caused by increased abrasion of the enamel coating of the dentition. In such situations, the boundary line requires covering with artificial crowns, which allow restoring the natural anatomical shape.
- Low location of the boundary line in the presence of cone-shaped elements, with the equator located at the cervical level. Involves the use of supporting structures.
Manufacturing: technology and materials
In orthodontics, clasp retainers are bent with forceps to obtain the required shape. Requirements for making a retainer:
- the shoulder should cover the cervical or vestibular part of the tooth,
- the shoulders should not pull or put pressure on the support unit,
- the clamp must touch the entire surface, otherwise the enamel will be erased at the point of contact,
- after production, polishing is required so as not to injure the mucous membrane,
- the shoulders should be elastic.
Depending on the material of manufacture, clasp clamps are:
- metal (more aesthetic, but less reliable),
- plastic (inferior to metal ones in reliability),
- combined.
In the production of nylon prostheses, it is possible to use clasps made of the same material. Such retainers are located near the gums, are practically invisible and do not damage the enamel.
Requirements for clasps
When choosing a fixation structure in the patient’s mouth, you need to take into account the requirements that it must fully comply with:
- type of fixation - materials must be the same for all supporting teeth;
- the prosthesis does not tip over or rotate after it is installed in the mouth;
- when closing the jaws and chewing, no injury to the supporting units occurs;
- preserving the aesthetics of a smile - metal hooks are unlikely to retain their beauty when installed on the front teeth.
Important! The purpose of clasps is to ensure the immobility of the prosthetic structure, but the doctor must take into account that they can be installed only if the units do not have pathological mobility (do not wobble) and have the correct anatomy of the coronal part.
How much does prosthetics cost?
The cost of prostheses with hook fixation is the lowest in the segment. For example, a “butterfly” prosthesis can cost from 6,500 rubles, a removable acrylic one from 15 thousand rubles. Much here depends on the length of the orthopedic structure, the type and material of the fastening, the number of clasps, and the base material.
1Glen P. McGeevey Partial Dentures, 2006.
Your questions and answers
QUESTION Hello, tell me, which prosthesis with clasps is better to install? Irina T.
ANSWER Hello, Irina. The choice of prosthesis will depend on the condition and number of supporting teeth, as well as the capabilities of the clinic and the patient’s preferences. With clasps you can make a removable partial denture, acrylic, Acry-free, nylon, acetal, or clasp denture. Better reliability and more compact sizes are found in classic clasp frames, as well as in their modern metal-free counterparts Quattro Ti (“Quadrotti”).
Author: Chernov A. R. (Thank you for your help in writing the article and the information provided)
What alternatives exist
An alternative to clasp fixation are attachments (clasps) and telescopic crowns. All of these options are used for removable dentures. Dentists note that orthopedic structures on attachments are fixed better, and they themselves are completely invisible from the outside. As for telescopic crowns, this is also a very good option, but it is considered the most difficult to manufacture.
“Mom wore a clasp denture for several years. It seemed convenient, but outwardly the metal hooks on the teeth stood out. Well, she began to smile less, of course, because of this. Then the prosthesis had to be changed, and the doctor persuaded me to use attachments. “He turned out to be much better in beauty, from the outside he looks like his own teeth and no hooks are visible.”
Lina O., review from the website stomatology.rf
If we consider the best option for prosthetics in principle, then here the first place is firmly held by dentures fixed on implants - fixed or conditionally removable. They have many advantages - strong, reliable and durable fastening, highest aesthetics, comfort when chewing (they feel like your “native” teeth).
Read on the topic: conditionally removable dentures on implants - how they are attached and how they differ from others.
NeoStom – Dentistry website
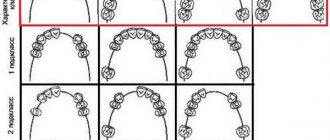
In addition to the clasps included in the Ney system, there are other varieties. All the different types of clasp fixation can be systematized depending on the design features of the holding arms of the clasps, i.e. directions of their retention endings.Types of clasps : The first group includes two subgroups of clasps with shoulders directed to the retention zone from the occlusion side, i.e. from the overlay. Most of them are relatively rigid clasp systems. The first group consists of double-armed and single-armed clasps. The second group includes clasps with shoulders directed to the retaining zone from the gum side. They are called rod clasps. They belong to springy (elastic) clasp systems.
The third group includes combined clasps, consisting mainly of the arms of the first and second groups, as well as a combination of rigid elements on the side of the occlusion and a wire arm. The first group - clasps with shoulders on the occlusion side, is divided into two subgroups: double-armed and single-armed. The first subgroup is double-arm clasps. The clasps belonging to this subgroup are built on the basis of the Acker clasp (Ney-I). Two-link (three-link) clasp. These are structures in which the vestibular and oral shoulders consist of several (2-3) links, with the last links on each side being retention ones. Due to the long length of the arms, they can be classified as flexible clasp systems.
Types of Acker clasp
a - two-link clasp; b - three-link clasp
There are cases when the tooth limiting the defect does not have a retention zone, but the adjacent tooth in front has a pronounced retention area. In such cases, two-link clasps are used. The first link is located on the tooth limiting the defect, above the boundary line, the second link is on the adjacent tooth below the boundary line, and the first link should be placed closer to the occlusal surface in order to cross the area of contact of both teeth without injuring the gingival papilla. Thus, the first links of the shoulders provide bilateral coverage of the tooth, and the second links provide retention. The three-link clasp is a combined design of a two-link clasp and an Acker clasp. Bonneville flip clasp. Reversible clasps include those structures that cross the occlusal surface in the transverse direction and are placed on the vestibular and oral sides of the abutment teeth. The Bonneville clasp is also called a double Acker clasp with arms directed in opposite directions. It is used on molars or on the second premolar and first molar with continuity of the dentition, for example, in Kennedy classes II and IV.
The upper or lower arches of the clasp denture are connected to the Bonville clasp using one connecting rod. In this case, the rod is placed vertically until it intersects with the boundary line, after which it continues into the gingival zone.
Bonneville switch clasp
The junction area of the four arms must be massive to withstand occlusal pressure. If there is no room to place the cast transverse parts of the clasp, then you can lightly grind the supporting teeth or antagonists for this. These clasps fill well the gaps (three spaces) between abutment teeth located at a small distance. In this case, they provide fixation of the prosthesis and are a contact point for adjacent teeth. In the Bonneville clasp, all four arms can be retaining, but it is possible to have two retaining and two stabilizing shoulders, located diagonally or bilaterally. Two occlusal pads on adjacent teeth provide sufficient support for the prosthesis and prevent the abutment teeth from moving apart (wedge-shaped action). In addition, occlusal linings prevent food from getting between the teeth. The Bonville clasp provides very good fixation, stabilization and support of the prosthesis, provided there is sufficient space between the antagonists. The embrasure clasp is a type of Bonneville clasp and also belongs to the reversible type. The clasp consists of two Acker clasps, having the opposite direction, in which the vestibular arms are shortened and look like hooks or hooks. They are placed in the occlusal zone and do not reach the boundary line. Consequently, they serve as stabilizing shoulders, and the two oral shoulders are retentive. If there are insufficient retention zones on the oral side, you should find corresponding retention zones on other teeth and additionally place clasps there.
Embrasure clasp
Embrasure clasps are also used for splinting mobile adjacent teeth. To do this, the oral arms of several clasps are connected to each other above the boundary line in a row of stabilizing arms. In this case, this system of clasps blocks all moving teeth and ensures their unloading from the vertical and horizontal components of chewing pressure. A double Acker clasp consists of two Acker clasps with shoulders directed towards each other. The two arms of this design are connected to form a two-link stabilizing arm, while the other two arms are retention arms. A clasp consisting of two opposing (oppositely directed) arms has two occlusal pads from which the arms extend. One or both shoulders may be retained. The clasp is used on single teeth when the retention zones are located diagonally. The arms of the clasp start from the medial and distal pads and are located depending on the boundary line on the vestibular and oral sides of the tooth. If one of the shoulders is stabilizing, then it is placed above the boundary line. The clasp can be used in one-sided dentures on the side of the continuous dentition.
a - double Acker clasp; b - clasp made of two opposing arms
Double clasp with occlusal pad on the adjacent tooth. A special feature of this design is the unusual arrangement of the main elements of the clasp on two teeth. In this case, the shoulders are placed on one tooth, used for coverage and retention, and the occlusal overlay is placed on the adjacent tooth, which is the supporting tooth. The mesio-distal clasp is used for splinting isolated anterior teeth with diastemas and trema. Such a clasp can be called a double-armed approximal clasp. Its shoulders cover the medial and lateral surfaces of the abutment tooth by more than 180°, which ensures fixation of the clasp.
The middle part of the clasp is supporting and is located above the guide line. Above the tubercle of the tooth, two short arms extend from it, with limited compliance. They should be placed in the gingival area almost under the very guide line, which makes their precise fit difficult. In order to strengthen the retention ends of the shoulders, they should be made relatively wide, but flat. When modeling a clasp, it should be kept in mind that the connecting rod must extend from the middle part of the clasp to contact the palatal plate, without touching the gingival margin.
a - two-arm clasp with an occlusal pad on an adjacent tooth; b — medio-distal clasp; c — shoulder-pin (“fish hook”) The use of mesio-distal clasps for the anterior teeth is advisable from an aesthetic point of view. However, placing the connecting rod in the middle of the oral surface of the tooth is their disadvantage, because there is a sensation of a foreign body interfering with the tongue. Shoulder stiletto. This name is due to the fact that one of the arms of the clasp has the shape of a hairpin. It is sometimes called a "fish hook". The clasp is used for use as retention of the near zone of the abutment tooth, i.e. in the case when, from the side of the defect, the boundary line approaches the occlusal surface. This occurs with medial inclination of single molars. Its retention arm (clasp) starts from the occlusal lining, with the covering part located above the boundary line, then the arm bends in the opposite direction, crosses the boundary line and ends in the retention zone. The clasp has a number of disadvantages that limit its use: • the shoulder covers a significant surface of the tooth, on which food can get stuck;
• elastic properties of the retaining end of the clasp arm are limited; • used only on molars. The second subgroup is single-arm clasps. Opposite rear action clasp (vestibular single-arm clasp). Considering the location of the connecting rod and the initial part of the clasp arm on the vestibular side of the dentition, it is advisable to call it a vestibular single-arm clasp. It is used in cases where the premolars on the lower jaw are inclined towards the tongue. Construction of prostheses using conventional types of clasp fixation is impossible, because on the vestibular side, premolars do not have a retention zone. On the oral side, on the contrary, there is a sufficient holding area, but there is no support zone that serves for the location of the rigid, enclosing elements of the clasp arms.
Opposite rear action clasp (vestibular single-arm clasp
The connecting rod starts from the area of the retention loops of the frame, does not touch the mucous membrane and, at the level of the abutment tooth, bends in the vertical direction until it connects with the clasp arm in the middle of the premolar. The vestibular part of the shoulder continues in the distal direction, in which the occlusal pad extends from it. This part of the shoulder is relatively rigid and provides coverage of the abutment tooth and stabilization of the prosthesis. It is used for Kennedy class I defects, providing a rational load on the supporting teeth, especially when they are mobile. The Swenson clasp is used on fangs. The occlusal pad is located on the medial side of the canine. The shoulder extends from the pad, curving down the tubercle and then up where it
Svenson clasp
near the cutting edge it passes to the vestibular surface and ends in the medio-vestibular zone. It is used for Kennedy class I defects, providing a rational load on the supporting teeth, especially when they are mobile.
Single-arm clasp with an occlusal pad on the adjacent tooth. If there is slight mobility of a tooth limiting a class I dentition defect according to Kennedy, it is not advisable to use it as support and retention. In this case, the clasp is placed on two adjacent teeth. A stable penultimate tooth is used for support, and a tooth limiting the defect in the dentition is used to fix the prosthesis on the jaw. The clasp arm covers the tooth on three sides and is elastic due to its large length.
a - double single-arm clasp for the upper jaw; b - double one-arm clasp for the lower jaw; c - single-arm clasp with an occlusal pad on the adjacent tooth. Double single-arm clasp for the upper jaw. It is used on the side of a continuous dentition, as well as with two isolated molars. The clasp is used when there is significant divergence of the molars, in which there is no retaining zone on the palatal side. The disadvantage of the design is the need for a gap between the premolar and molar to position the front arm of the clasp with a continuous row of teeth. Double one-arm clasp for the lower jaw. Used when there are two converging molars. It is similar to the previous system, but the condition for its use is the presence of favorable areas on the vestibular side of the alveolar process for the location of the connecting rod. Due to the lingual inclination of the two molars, both arms begin on the labial side, continue on the proximal sides, and end at the retentive ends near the contact of both molars.
Modifications of Roach's clasp.
a — C-shaped rod shoulder; b - i-shaped rod shoulder; c — L-shaped rod arm The clasp design is shown in the presence of converging four molars on both sides of the dentition, for example, 87178.
This subgroup also includes clasps of the Ney system: rear-action clasp (Ney-IV) and ring clasp (Ney-V). The second group is clasps with shoulders on the gum side (rod clasps). In their structure, the clasps of this group have elements of the Roach clasp (Ney-II). Thanks to the elongated arms, these clasps are classified as flexible (springy) clasp systems. They are sometimes called load crushers because... the elasticity of the clasp arms helps reduce the effect of the horizontal component of the chewing load on the supporting teeth. This group includes clasp systems with two rod arms on the oral and vestibular sides. Roach clasp with modified shoulder. The classic Roach clasp is used most often on single molars of both jaws. However, depending on the position of the tooth, different types of rod arms of clasps are used on the vestibular and oral sides, and the arms are designated by letters whose shape they resemble (C, G, i, T). When the gripping area on the supporting tooth is distant from the base, a rod shoulder is used, shaped like a horizontal letter “L”. If the grip zone is adjacent to the base, then a C-shaped rod arm can be used.
a — T-shaped arm of the Roach clasp; b — T-shaped rod arm of Bonigard
The retention areas of these shoulders have a small area of contact with the gingival zone of the abutment tooth. The fixation of the clasps can be increased by giving the ends of the rod arms a T-shape. The third group is combined clasp systems. If in the Acker clasp and its modifications both arms can be functionally retaining, or one of them is retaining and the other is stabilizing (reacting), then in combined clasps, which are a combination of the shoulders of the first and second groups, only one shoulder is retentional, and the second is always counteracting (stabilizing). Along with Roach, a number of authors point out the possibility of using small retaining areas near the neck of the tooth to retain the arms of clasps, for example, on canines and premolars that have a poorly defined equator on the vestibular side. Currently, the cast Bonigard rod arm is used, which, like the T-shaped arm of the Roach clasp, belongs to the split clasp systems. The T-shaped end of the Bonigard rod arm is placed entirely in the gingival zone, between the boundary line and the gingival margin. The Bonigard clasp is used only on the front teeth or premolars. In contrast, the T-arm of the Roach clasp is used on molars. It has a more elongated split part, which is located almost along its entire length on the vestibular or oral sides of the molar. Clasps of the third group are divided into two subgroups. The first subgroup includes clasp designs with one arm on the occlusion side and a second rod arm on the gingival side. The second subgroup also includes clasps with one arm on the occlusion side and a second wire arm. The first subgroup is clasps with one rod arm. A clasp with Acker and Roach shoulders (Ney-III) is described in the section “Clamps of the Ney system”. Double split clasp. This clasp design uses two supporting teeth. The retention part consists of two split shoulders located in the gingival zones of the teeth. The stabilizing arms of the clasp are also located on two teeth in the occlusal zones, i.e. above the boundary line. The clasp is used on the front teeth and premolars and ensures reliable fixation of the prosthesis.
Clasp with Acker and Bonigard shoulders. The clasp has on one side a long elastic retention arm of Bonigard, and on the other side it is opposed by a second, shorter and more pliable Acker's opposing arm, which protects the abutment tooth from displacement. The latter must cover the oral half of the tooth to ensure stabilization of the denture. Used on anterior teeth and premolars.
Clasps with one rod arm.
a - double split clasp; b - ring clasp and Bonigard shoulder; c - clasp with Akker and Bonigard shoulders; d — ring plummer and Bonigard shoulder; d - clasp with Acker shoulder and Fera rod shoulder. Oral lining and Bonigard shoulder. On the lingual (palatal) side of the front teeth there are multi-link onlays, and on the vestibular side of the abutment tooth, in the gingival zone, there is a Bonigard rod shoulder. Ring clasp and Bonygard shoulder. This combined clasp is used on single small premolars of both jaws, when the retention arm of the ring clasp, due to its short length, cannot provide elasticity. In this case, a Bonygard holding rod shoulder is used in combination with an opposing rigid shoulder and two pads. The latter are connected with the help of branches to the frame on the upper jaw or to the clasp on the lower jaw. Clasp with Acker shoulder and Fehr rod shoulder. In this system, the end of the rod arm in the shape of a half ring, located in the gingival zone of the canine or premolar, is the retention end. This half-ring is connected to a support rod, which is loop-shaped to provide elasticity to the shoulder. The rigid Acker arm serves as a counteraction in the clasp, covering the tooth from the oral side and connecting to the occlusal pad. When modifying the Fehr design, it is possible to use a vestibular rod shoulder together with an Acker shoulder, an oral lining, or a ring clasp, i.e. in the same combination as when using the Bonigard rod arm.
The second subgroup is clasps with one wire arm. Acker shoulder and wire shoulder. In this system, the retentive arm is the wire arm, and the counteracting arm is the Acker arm. The wire shoulder absorbs functional loads before the supporting tooth receives them. It can be soldered to a frame made of a cobalt-chromium alloy or cast together with a frame made of a gold-platinum alloy, and can be attached to the base in the usual way. The most rational is the use of wire clasps for class I dental defects according to Kennedy. Oral pad and wire shoulder. In this system, the retention arm is the wire arm, and the stabilizing arm is the oral (palatal, lingual) pad. In class I dentition defects, when multi-link onlays are used on all remaining teeth, wire shoulders are located on the vestibular side of the supporting teeth, which well fix the prosthesis on the jaw. Ring clasp and wire arm. This clasp is used on single premolars or molars, when, due to the small vestibular curvature of the abutment tooth, it is necessary to use a wire arm that secures the prosthesis well. In addition, the clasp is used to transfer the load along the axis of the abutment tooth. To do this, two pads are placed on it, and to reduce the horizontal component of the chewing load, a pressure distributor in the form of a wire arm is used.
Clasps with one wire arm.
a - Acker shoulder and wire shoulder; b — oral lining and wire shoulder; c - ring clasp and wire arm The choice of clasp is influenced by the position of the boundary line identified during parallelometry. There are five main types of boundary lines that are more common. 1. The boundary line runs in the middle of the approximal line and rises along the vestibular surface of the tooth to the contact point with the adjacent tooth. This arrangement of the equator line will allow you to conveniently place the Acker support-retaining clasp on the tooth.
2. The boundary line begins at the level of the contact point of the tooth on the side of the dentition defect and along the vestibular surface descends to the middle of the proximal surface of the adjacent tooth. In this case, it is recommended to use clasps with long retaining arms, Roach clasps, Bonigard clasps. 3. Diagonal location of the equator on the supporting tooth. The equator passes near the chewing surface in the area of the dentition defect, obliquely crosses the vestibular surface of the supporting tooth and ends at the neck of the tooth on the opposite side. If it is a premolar, then a type 4 clasp according to Ney’s classification is used, and if it is a molar, a Ney ring clasp is used. Both clasps have long arms; due to their elasticity, they easily pass the equator of the abutment tooth, providing good fixation of the prosthesis and transmission of chewing pressure along the axis of the tooth. 4. When teeth are worn out, the equator is located high, it passes at the level of the chewing surface. Such teeth need to be covered with artificial crowns that restore their anatomical shape. 5. A low outline of the equator line is found in teeth that have the shape of a truncated cone. The equator passes at the level of the tooth neck. Such a tooth can only be used for a supporting clasp, otherwise it is necessary to restore its anatomical shape with a crown. Clinical and functional requirements for the natural tooth crown selected for the location of the support-retaining clasp: 1. The tooth must be stable. In case of pathological mobility of teeth, they should be blocked with adjacent teeth to form a stable system. Teeth with chronic periapical inflammatory foci can be used for support only after successful root canal filling.
2. Teeth must have a distinct anatomical shape. Teeth with a low cone-shaped crown, exposed neck and a sharp violation of the ratio of the length of the clinical crown and root are unsuitable for clasp fixation. These disadvantages are relative contraindications. After special preparation, such teeth can be included in the support of the clasp system. 3. It is necessary to take into account the relationship of the supporting tooth with the antagonist. This relationship can be so close that even a small occlusal pad placed in a fissure on the occlusal surface will disrupt the bite. In such cases, you should choose another tooth to place the supporting element or make a crown on the supporting tooth.
You might be interested in:
- Arch of a clasp prosthesis
- Telescopic fixation system
- Beam fixation system
- Locking system
- Anchor fixation system
Related materials:
- Ney system clasp
- Clasp structure
- Planning the design of a clasp prosthesis
- Prosthetics with clasp dentures
How to care for your prosthesis
Any dentures require careful and daily cleaning. For care, it is recommended to use a toothbrush with soft bristles and toothpaste without abrasive particles. Within a minute, all parts are cleaned with light movements without pressure until foam forms. After rinsing with clean water, you can additionally treat with an antiseptic solution or mouth rinse.
As an additional disinfection, you can use special containers with ultrasonic cleaning. The device generates a large number of air bubbles, which gently remove plaque and prevent unpleasant odors. Dentists do not recommend leaving the denture in the mouth overnight: this can cause metal oxidation.
Advantages and disadvantages
Hook dentures, as mentioned, are one of the common ways to restore jaw functionality. The main advantages of the design are long service life, reliability, and efficiency during everyday wear.
Products are recommended for partial or complete loss of teeth. Unlike acrylic structures, the clasp system is based on a metal frame. Artificial teeth are attached to it. The structural features lead to a reduction in the weight and size of the product, which increases its significant characteristics.
The main advantages of the clasp prosthesis:
- the process of soft tissue atrophy is not as fast as when using acrylic products. When the service life of the structure expires, the patient will feel discomfort,
- The reduced size of the system increases ease of use. Instead of a polymer arc, a metal alloy is used, which improves diction, the ability to clearly distinguish tastes, and move the tongue freely. There is no risk of artificial teeth falling out,
- the metal frame increases the reliability of the system, the risk of breaking is minimal,
- The service life is much longer than that of classic products. If you perform proper hygiene and follow the doctor’s advice, dentures last 5 years instead of the usual 2.5,
- the price is affordable for different segments of the population. Although the cost is higher than acrylic structures, the benefits are worth the cost.
Complications that may arise due to clasps
Negative consequences or complications associated with prosthesis attachments can occur for various reasons. These include low-quality materials, errors at the manufacturing or installation stage, and non-compliance with operating rules. You may also be allergic to metal or synthetic materials. In patients who already have dentures made of other metals in their mouths, galvanosis often occurs - the sensation of an electrical impulse. Often chips and cracks appear in the enamel, gums bleed and recede, and the necks of the teeth are exposed.
If oral hygiene is unsatisfactory, pieces of food become trapped under the hooks, plaque and tartar form. This provokes caries, periodontitis, causes an unpleasant odor and generally worsens the aesthetics of a smile.
Possible consequences
Failure by a specialist to comply with the technology for manufacturing clasps for removable dentures threatens the patient with a lot of inconvenience.
Here are the main ones:
- deterioration of the condition of supporting teeth due to a decrease in the quality of bacterial plaque removal, which is fraught with the development of caries and destruction of elements;
- severe abrasion of enamel as a result of regular increased load;
- loosening of teeth due to overload caused by horizontal movements of the prosthesis.
Manufacturing Basics
The production of bent-type support-holding clasps is carried out using special pliers, pliers or round-nose pliers
- Using pliers, bends one of the ends of the wire to form the shoulder of the product.
- Performs a second bend that forms the body of the clasp.
- Forms an extension of the retainer thanks to the third bend of the steel wire.
Double-armed products are made in an identical way with the formation of two elements.
Features of the production of the shoulder and contact process
When making a shoulder, the technician must follow several important rules. The element should be designed so that it meets the following requirements:
- covered the tooth from the labial or cervical area;
- did not exert pressure on the supporting element of the row;
- was carefully polished to avoid damage to the oral mucosa;
- touched the tooth surface as much as possible;
- had sufficient elasticity.
When making a contact process, the technician must use several tools: round-nose pliers to fix the shape, pliers to make a bend to the ridge.
For strong bonding with the base, the workpiece is crushed on an anvil and covered with notches.
The video shows the manufacturing process of Jackson clasps.