Why does gum recession develop?
Recession can be either an independent disease or a symptom that accompanies a certain pathology. It occurs for various reasons:
- Improper hygiene procedures. If you brush your teeth with a hard brush or press hard on it, you can damage the tissue. As a result, inflammation develops and the periodontal structure is disrupted.
- Bad habits. Smoking causes blood vessels to narrow because they are exposed to toxic substances from tobacco smoke. In this case, the blood supply is disrupted, which provokes tissue sagging.
- Bite pathologies, dentition defects. In such cases, the chewing load is distributed unevenly. Therefore, on the one hand, the dental system experiences increased stress, crowns wear off, and gums recede.
- Anatomical imperfections. With a shortened frenulum of the tongue, upper and lower lips, a small vestibule of the oral cavity, short strands of the mucous membrane, as well as in the case of other disorders, recession may occur.
- Incorrect prosthetics. If the gums recede only in the area of the crown, this symptom often indicates an allergic reaction to the materials used to make the dentures, or its incorrect installation.
- Errors when implanting orthodontic structures. If a patient's teeth quickly shift while wearing braces, this causes excessive pressure on the gums, which exposes the roots.
- Age-related changes. People who have reached older ages are more susceptible to the disease.
- Vitamin deficiency, in particular lack of vitamin C.
Regardless of the causative factor, treatment must be started as quickly as possible. Only a doctor can tell you what to do in each specific case.
Causes of receding gums
If the gums have receded onto the tooth, this may indicate a dental disease that has caused thinning and reduction in the volume of soft tissues.
In most cases, the causes of gum recession are:
- neglect of hygiene - with irregular cleaning, tartar forms in the oral cavity, causing inflammation of the gums and their decline;
- mechanical trauma to the gingival tissue (for example, during brushing your teeth or while eating);
- gum atrophy caused by natural aging of the body;
- injuries during treatment, implantation or teeth whitening, as a result of which an inflammatory process developed;
- advanced or severe periodontal disease, accumulation of pus in periodontal pockets;
- incorrectly or poorly made dentures that rub soft tissues, errors in orthodontic treatment;
- anomalies and defects of bite;
- pathologies of the structure of the mucous membrane, in which the gums are initially thin and weakened;
- excessively thin cortical bone, causing circulatory problems;
- general diseases of the body that impair blood circulation and the functioning of the immune system.
Only a dentist can determine the exact reason why the gums on the teeth recede, so at the first signs of recession you should contact the clinic.
Clinical picture during the development of recession
As the disease develops, the gums on the lower teeth recede and those on the upper teeth rise. The roots are gradually exposed. They are not covered with enamel, as a result of which they lack protection. Because of this, tooth sensitivity increases. Visually they look elongated, their color changes at the gums. Interdental gaps form, in which food constantly gets stuck, which brings a lot of inconvenience. In advanced cases, bleeding appears and the gums become inflamed.
The pathology can be localized, that is, affect 1-2 teeth, or generalized, when the entire dentition is involved in the painful process.
Surgery
In case of severe gum loss, the only effective way to restore it is soft tissue surgery. Today, several surgical techniques are actively used.
| Methodology | Description |
| Flap reconstruction | Gum plastic surgery, when its deficiency is compensated with the help of a donor flap, which is taken from neighboring areas. If the patient’s gums have dropped slightly (by 2-3 mm), this method can be used to quickly restore its previous level. Disadvantages of the technique are traumatic and aesthetic defects (there may be a discrepancy in color between the donor and native areas) |
| Tissue regeneration using plasma lifting and PRF membranes | A more modern technique that does not require taking donor tissue. Injections of plasma and/or installation of fibrin membranes are made into the affected area. This starts the process of tissue regeneration. The treatment is longer compared to the first method, but it is effective and less traumatic |
| Installation of a collagen implant | A minimally invasive technique that is effective for tissue restoration after periodontal disease or age-related gum atrophy. Such implants contain an analogue of connective tissue, which helps restore gums |
| Classic implantation | What to do if the gums have receded, the tooth root is exposed, and the doctor says that tooth extraction is no longer possible? The best solution in this case would be bone grafting and the installation of dental implants. This is the only way to effectively replace lost teeth. In some situations, additional soft tissue plastic surgery may be required. |
In case of mechanical damage, receding gums can be raised using classic surgery with sutures. This is only possible if there are no serious injuries that require additional measures. It is important that surgical treatment is also aimed at eliminating visual defects. To deal with the root cause, comprehensive treatment is required, especially in cases where periodontal diseases develop against the background of problems with the functioning of other body systems.
What is the problem?
Because the part of the tooth that is not covered by enamel is exposed, the risk of developing root caries increases. In this case, it is difficult to cure, since ensuring a high-quality fit of the filling material to the root tissues is very problematic due to their hydrophilicity. Over time, teeth can become loose because there is not enough tissue available to hold them in place.
In addition, gum recession is an aesthetic problem, especially when the disease is advanced. People suffering from the disease develop complexes, which leads to social isolation.
Doctor's mistakes leading to loose gums
With the cement method of fixation, the following problems may occur:
- The solution gets into the space between the gum and the abutment . Fastening is accompanied by squeezing out excess solution, which neither the doctor nor the patient can control. Attempting to remove excess cement may damage the surface of the implant. The process threatens with inflammation of the bone tissue - peri-implantitis. In the worst case, loss of the structure or part of the bone tissue is possible.
- Minor errors when taking an impression and making a prosthesis . If the crown does not contact the abutment tightly enough, the cement mortar will be eroded by saliva. This will lead to the formation of soft plaque. It contains pathogenic bacteria that can cause peri-implantitis. The cemented crown will fall out.
The use of dental cement allows for the correction of errors. Screw fixation does not provide this option. Violation of the protocol for fixing the prosthesis using a screw method is fraught with rupture of the fasteners. It will need to be removed from the implant, which is not easy to do.
Diagnosis of gum recession
First, the doctor will conduct a visual examination and collect anamnesis. This may be enough for a specialist to make a diagnosis. To confirm it, the following studies are additionally prescribed:
- CT scan;
- inoculation of smears taken from the oral cavity to establish pathogenic microflora;
- clinical tests that are aimed at determining mineral deficiency.
Only after a thorough diagnosis will the dentist recommend how to treat the pathology.
Prevention of gum recession
- Don't start caries. Place high-quality fillings in a timely manner and prevent the appearance of cervical caries.
- Keep your mouth clean. Follow your teeth brushing technique.
- Have your hair professionally cleaned at least once every six months.
- Avoid injury.
- Massage your gums regularly.
- Take mineral-vitamin complexes with vitamins A, D and group B.
Do not forget that at an early stage it is easier, faster and cheaper to cure the disease. Therefore, consult a doctor as soon as you notice its first signs.
What treatment methods are used for receding gums?
Can gums heal on their own? Unfortunately no. But stopping the pathological process is quite possible. Treatment is a rather complex undertaking that requires an integrated approach. In addition, it is not always possible to guarantee a 100% result.
At the initial stages of treatment, it is important to eliminate the cause that caused the gums to recede. In this case, physiotherapeutic procedures, oral hygiene, correction of orthodontic or orthopedic structures, prosthetics, plastic surgery of frenulum, cords, and vestibule of the oral cavity are carried out. If the deviations are caused by a malocclusion, the orthodontist carries out appropriate treatment, which may take several years, but only in this way will the root cause be eliminated.
How to deal with the disease is determined depending on the degree of neglect of the problem. Different techniques can be used:
- Drug therapy. It helps only in the initial stages of the development of the disease. It is aimed at combating concomitant periodontal pathologies, somatic diseases, and helps strengthen the gums and exposed areas of the teeth. Patients are prescribed immunomodulators, anti-inflammatory, hormonal agents, and vitamin complexes.
- Cleaning and polishing of tooth roots. It is carried out in several stages. First, the doctor removes dental plaque above and below the gum, after which he polishes the roots. Thanks to such actions, the gums will be able to “fix” to the surface of the teeth again.
- Gum plastic surgery. The operation is performed using different techniques. The flap method involves cutting the gums. The resulting flap is lifted to gain access to the roots, which are cleaned and polished. The gum is then reattached to the tooth. In some cases, regenerative materials such as membrane, a protein that has the ability to stimulate tissue, are used. When the loss of gum tissue is large, to restore it, the doctor may recommend transplantation (a section of the mucous membrane is taken from the upper palate and transferred to the problem area).
How to lift the gums is determined in each individual case by the doctor, carefully analyzing the clinical picture.
Symptoms and forms of the disease
Today, when diagnosing the severity of the disease, the Miller classification is used, which involves 4 stages of gum recession.
- Visually, gum loss is hardly noticeable (or completely unnoticeable) and appears only in the area of contact between the tooth and gum.
- The defect appears slightly in the area of contact between the gum and the neck of the tooth (the level of the attached gum decreases by 1-2 mm). The gums between the teeth remain at the same level.
- The gums recede by 3 mm or more. The necks of the teeth are slightly exposed, but the bone level does not decrease. At this stage, the gums often recede and bleed.
- The most severe stage, when the gums recede by 5 mm or more, the roots of the teeth become visible. Mobility of the teeth is observed, which at this stage of the pathology is often generalized and involves several teeth.
At advanced stages, pathology can be noticed visually, especially when the gums on the front teeth recede. If the pathology is at the beginning of its development, a number of additional symptoms help to detect it.
- Inflammatory process, bleeding.
- Formation of periodontal pockets.
- The sensitivity of the enamel has increased.
- The presence of a thick layer of dental plaque.
- Unhealthy whitish tint of gums.
Only a doctor can make an accurate diagnosis (using modern technologies), so if you have at least one symptom, you should not postpone your visit to the clinic. Of course, everyone is interested in the question of what to do if the gums on a tooth have receded and what treatment should be chosen. There are two directions: therapeutic and surgical. The choice depends on the severity of the pathology and the underlying disease that led to soft tissue atrophy.
Unusual gum enlargement: clinical case
Gingival fibromatosis, gingivomatosis, diffuse fibroma, elephantiasis, idiopathic fibromatosis, hereditary gingival hyperplasia, gingival gigantism and gingival hypertrophy are variants of slowly developing fibrous growths of the gums on the upper and lower jaw.
Gingival fibromatosis can be due to hereditary causes, also associated with taking medications, or idiopathic. Also, this pathology can be caused by inflammation or leukocyte infiltration.
Gingival fibromatosis is found as an isolated lesion or associated with a more serious hereditary syndrome, for example, Rutherford syndrome, Jones syndrome, Murray-Puretic-Drescher syndrome, Laband syndrome, Ramon syndrome, hypothyroidism and other pathologies. Most often, hypertrichosis is combined with a hereditary form of gingival fibromatosis. This form of pathology is characterized by massive enlargement of the gums, which covers all surfaces of the teeth. Enlargement may be associated with one or more teeth, involving one or more quadrants, or as a generalized form. The cause of this proliferation remains unknown, but there is evidence of a genetic predisposition.
Gingival hyperplasia creates favorable conditions for the accumulation of plaque in deep gingival grooves. Secondary inflammatory processes aggravate existing gum hyperplasia.
Aggressive periodontitis is a genetically inherited disease that is manifested by severe and rapid progression of damage to periodontal tissue. This form of periodontitis clinically looks very special, often occurring during puberty in the absence of obvious local factors, such as a large amount of plaque and tartar.
Aggressive periodontitis is characterized by the following features:
1. Clinical manifestation at a young age 2. Unremarkable history 3. Rapid loss of epithelial attachment and bone destruction 4. Familial pattern
This article demonstrates a rare case of asyndromic idiopathic gingival enlargement associated with aggressive periodontitis and its treatment.
Clinical case
A 20-year-old man came to the clinic with complaints of swelling of the gums near the left upper and left lower teeth, as well as the inability to chew food on the left side. The patient had a history of facial trauma on the left side about three months ago, after which gum swelling first appeared, which gradually increased in size to its present appearance. However, no relationship was found between trauma and gingival overgrowth. The patient sought help only when the gums began to interfere with chewing. The patient's medical history is unremarkable. Family history information was missing.
On intraoral examination, the gums on the left looked noticeably enlarged. Gingival growth extended from the first premolar to the second molar in both jaws (Photos 1 and 2). The formation was dense and fibrous, accompanied by an inflammatory component, possibly due to the inability to maintain adequate personal oral hygiene. Gingival growth was located from the buccal to lingual and palatal mucosa of the oral cavity. The diffuse type of formation involved the marginal, interdental and attached gingiva. Periodontal probing revealed deep pockets near the involved teeth. Mobility of all involved teeth was present.
Photo 1: Gingival hyperplasia on the left of the upper jaw
Photo 2: Gingival hyperplasia on the left of the lower jaw
X-ray examination
OPTG revealed the presence of remaining bone in the amount of 30 to 35% on the left in both jaws. A severe form of bone loss was recognized on the left upper and lower jaw (Photo 3).
Photo 3: OPTG
Hematological examination
Standard hematological examination revealed hemoglobin 12.6% and polymorphonuclear leukocytes 75%, lymphocytes 23%, monocytes 0%, eosinophils 2%, basophils 0%.
Histological analysis
An incisional biopsy showed layered epithelium covering the connective tissue stroma. In some zones there was flattening, in others - elevation. The connective tissue is densely collagenized and filled with oval and spindle-shaped fibroblasts. The section contained several chronic inflammatory cells, mainly consisting of lymphocytes. Blood vessels with endothelial lining of small and medium diameter were also found.
Based on the above signs, a diagnosis of gingival fibromatosis associated with aggressive periodontitis was made.
Treatment
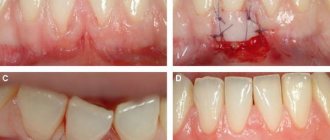
Initial therapy is based on standard periodontal treatment. Overgrown tissue is removed by external gingivotomy under local anesthesia. The operation was carried out in two stages, the left maxillary part was involved in the first stage (Photos 4 and 5) and the left mandibular part in the second (Photo 6). The interval between the two interventions was 3 weeks. A periodontal bandage was made. Antibiotics, B-complex drugs and anti-inflammatory agents are prescribed for one week.
Photo 4: Operation (upper jaw)
Photo 5: Operation (upper jaw)
Photo 6: Operation (lower jaw)
Postoperative healing was uneventful. The periodontal dressing was removed after one week. The surgical area is flushed generously with betadine and saline. Recommendations for the postoperative period are given, the patient is scheduled after one week and then after a month to evaluate the results. Healing occurred uneventfully after one month (Photos 7 and 8). The patient is satisfied with the result.
Photo 7: One month after surgery (upper jaw)
Photo 8: One month after surgery (lower jaw)
Photo 9: Microspecimen
Discussion
Gingival fibromatosis is often associated with various syndromes, such as Ruthenford, Laband, Cross, Murray-Puretic-Drescher, Jones syndrome, hypertrichosis and epilepsy. Also, the causes may be many factors, including inflammation, leukocyte infiltration, taking medications such as phenyton, cyclosporine and nifedipine.
This article demonstrates a clinical case of severe gum overgrowth on the left side of both jaws. A blood test revealed no pathology. Clinical and histological features, as well as systemic examination, ruled out neoplastic growth. Gingival hyperplasia occurs in some patients while taking phenyton, cyclosorine and nifedipine. The study patient did not take any of these drugs.
The patient did not have any symptoms of mental impairment. He did not suffer from epilepsy or hypertrichosis, and there were no tumors or corneal degeneration. No skeletal deformities, skin or nail pathologies were detected. Thus, the association of the syndrome with the specified gingival growth was unlikely.
In most forms of gingival enlargement, rapid loss of alveolar bone or epithelial attachment is not common. However, this patient experienced progressive destruction of periodontal tissue. Loss of alveolar bone was evident on X-ray analysis. There was little inflammation despite deep periodontal pockets and extensive bone loss. The amount of plaque on the affected teeth was minimal, which did not correspond to the level of bone destruction.
In this clinical case, we observe a young man, 20 years old, with an uncomplicated medical history and a severe form of bone tissue destruction, consistent with the diagnosis of aggressive periodontitis. No clear information was available regarding family history.
This case was first reported in 2004 by Casavechia. Until 2004, no such case was mentioned. Historically, gingival fibromatosis has always been associated with various other syndromes and disorders and has never before been described in association with aggressive periodontitis. Genetic analysis as well as analysis of neutrophil function have been performed, but no single mechanism has been identified.
Since Casavechhia, three more such cases have been described in which nonsyndromic idiopathic gingival overgrowth occurred associated with generalized aggressive periodontitis.
Aggressive periodontitis is typically characterized by a hereditary nature, which was established by segregation analysis of affected families. Mendelian inheritance has been established, and therefore autosomal (dominant and recessive) as well as X-linked inheritance has been proposed. Based on the data obtained, the patient was diagnosed with generalized periodontitis with idiopathic gingival fibromatosis.
The results of histological examination revealed signs of fibrous gingival hyperplasia, as evidenced by thickening of the acantholytic epithelium with an elongated margin and dense saturation of collagen with a large number of fibroblasts, as well as neovascularization in some areas.
Treatment varies depending on the severity of the condition. When overgrowth is minimal, careful scaling and good personal oral hygiene are recommended. A relative increase in gingival mass requires surgical intervention. In the past, treatment included removal of all involved teeth and reduction of the alveolar margin. Many techniques have been used to excise enlarged gingiva, including internal and external gingivotomy in association with gingivoplasty, apical positioning of the flap, electrocautery, carbide bur in a turbine tip, and CO2 laser. However, among the entire list, standard external gingivotomy remains the most common. Relapse with this pathology often occurs at different time intervals. In several reported cases, relapse did not occur for 2, 3, or even 14 years.
For this case, external gingivotomy was performed under local anesthesia on the upper and lower jaws. Healing proceeded without any problems, the patient was satisfied. The patient was warned about a possible relapse and was also instructed on hygiene measures.
Conclusion
This article describes a rare case of a combination of gingival overgrowth and generalized aggressive bone destruction. The diagnosis was based on clinical, radiological and pathohistological studies. However, to establish the relationship between the two pathologies, it is necessary to conduct a more in-depth analysis, including immunological and genetic tests.
Authors: Ashutosh Dixit , Department of Periodontics, Seema Dental College, Rishikesh, India Seema Dixit , Department of Conservative Dentistry and Endodontics, Seema Dental College, Rishikesh, India Pravin Kumar , Department of Conservative Dentistry and Endodontics, Seema Dental College, Rishikesh, India
How is the recovery period going?
The period of complete healing of the gums after gingivoplasty depends on the method used and the complexity of the operation. On average, recovery lasts about one and a half to two weeks. To prevent complications, it is important to follow your doctor’s recommendations:
- Leave the oral cavity at rest for 6–10 hours. To do this, do not eat food for the time specified by your doctor.
- Quit smoking for at least three days, and even better until complete healing.
- Take all medications prescribed by your doctor.
- Use a special mouth guard to protect the operated area.
- Avoid foods that are hard or irritating to mucous membranes.
- Brush your teeth as usual, without touching the area where the plastic surgery was performed.
- Do not overwork, limit physical activity.
After gingivoplasty, the quantitative characteristics of the mucous membrane gradually return to normal. The gingival margin fits more tightly to the implant, and the restored area takes on an aesthetic appearance.