Anti-inflammatory drugs are drugs from different pharmacological groups that inhibit the development of inflammation.
Inflammation is a kind of protective reaction of the body in response to damage to cells and tissues caused by pathogens (viruses, bacteria, fungi, protozoa), injury, burns, etc. The entire process of inflammation is aimed at removing an unfavorable factor from the body, preventing deeper cell damage and restoring the integrity of the affected tissues.
However, excessive inflammation leads to metabolic disorders, decreased nutrition (trophism), oxygen starvation (hypoxia) and ultimately the death of the affected tissues.
Almost any human disease occurs with the development of inflammation, which varies in the mechanisms of development, severity and characteristics of the course.
Indications for use
Anti-inflammatory drugs are indicated for conditions that are accompanied by severe inflammation: autoimmune connective tissue diseases - rheumatoid arthritis, juvenile rheumatoid arthritis, psoriatic arthritis, systemic lupus erythematosus; inflammatory bowel diseases (nonspecific ulcerative colitis, Crohn's disease).
Glucocorticoids are additionally used for severe allergic conditions - anaphylactic (allergic) shock, Quincke's edema, bronchial asthma, allergic dermatitis; for severe skin diseases (psoriasis); with a sharp drop in blood pressure - cardiogenic, traumatic, toxic shocks; autoimmune kidney disease – glomerulonephritis; for blood diseases - leukemia, aplastic anemia; as well as for traumatic brain injury, cerebral and pulmonary edema.
Certain anti-inflammatory drugs (glucocorticosteroids, methotrexate, azathioprine) are used after organ and tissue transplantation to prevent their rejection, as well as in the treatment of malignant tumors (cancer).
Nonsteroidal anti-inflammatory drugs are used for inflammatory diseases of the joints (osteoarthritis, arthrosis); injuries to muscles, joints, ligaments; headache, menstrual, dental, muscle and joint pain; pain after injuries and operations; elevated body temperature with bronchitis, pneumonia, rhinosinusitis, sore throat, otitis, acute respiratory viral infections, etc.
How and why does the inflammatory process occur in the human body?
Inflammation is the body's defense method, allowing it to eliminate germs, harmful substances and dead cells. The inflammatory process can begin due to many reasons, including infections caused by bacteria and viruses, the action of chemicals, and also as a result of foreign bodies entering the body.
Inflammation can be acute or chronic. In the chronic form it occurs more slowly and for a long time. The main symptoms of the inflammatory process are redness, swelling, pain, fever and loss of certain functions.
pharmachologic effect
Anti-inflammatory drugs inhibit inflammation by blocking enzymes that are involved in the formation of special inflammatory factors - prostaglandins: glucocorticosteroids inhibit the enzyme phospholipase A2, non-steroidal anti-inflammatory drugs - the enzyme cyclooxygenase-2.
Glucocorticoids additionally have an antiallergic, immunosuppressive (immunosuppressive) effect, increase blood pressure (anti-shock effect), and activate the liver’s ability to neutralize toxins (antitoxic effect).
In addition to their anti-inflammatory effect, non-steroidal anti-inflammatory drugs also have the ability to reduce pain (analgesic effect) and reduce elevated body temperature (antipyretic effect).
Antirheumatic drugs have an anti-inflammatory and immunosuppressive effect due to inhibition of the formation of specific signaling molecules responsible for the implementation of inflammation - cytokines: tumor necrosis factor-α, interleukin-1 receptors.
How to take anti-inflammatory medications correctly?
First you need to carefully read the instructions. The drugs must be prescribed by the attending physician and the optimal dose and course of treatment determined. To protect the stomach, tablets should be taken with a sufficient amount of clean water.
Under no circumstances should you mix medications with alcohol. This will further affect the functioning of the stomach.
You can buy all drugs for the treatment of inflammatory processes in the network of state pharmacies “Provincial Pharmacies”. We provide medicines with a state quality guarantee. There is a pick-up system and home delivery when ordering drugs online.
Classification of anti-inflammatory drugs
Anti-inflammatory drugs are classified into:
- Antirheumatic drugs: aminoquinolines (hydroxychloroquine, chloroquine);
- gold preparations (auranofin, aurothioglucose, sodium aurothiomalate);
- tumor necrosis factor-α inhibitors (etanercept, infliximab, adalimumab, golimumab);
- interleukin-1 receptor antagonists (anakinra);
- others (leflunomide, methotrexate, azathioprine, penicillamine, sulfasalazine).
- non-selective inhibitors of cyclooxygenase-1 and cyclooxygenase-2 (acetylsalicylic acid, ibuprofen, naproxen, ketoprofen, flurbiprofen, dexibuprofen, dexketoprofen, diclofenac, indomethacin, aceclofenac, mefenamic acid);
Most herbal medicines (chamomile, sage, eucalyptus, linden, thyme, plantain, marshmallow, licorice, oak, milk thistle, etc.) have an anti-inflammatory effect, due to the presence of flavonoids, essential oils and tannins in their composition.
Anti-inflammatory drugs that act only in the bronchi include the leukotriene receptor blockers montelukast and zafirlukast.
Preparations of quercetin, glucosamine (hydrochloride and sulfate), and chondroitin sulfate also have an anti-inflammatory effect.
What non-steroidal anti-inflammatory drugs are most often prescribed for arthrosis?
- Aspirin is indicated in the initial stages of treatment of arthrosis and osteoarthritis, however, patients with diseases of the heart, blood vessels and gastrointestinal tract require special caution.
- Diclofenac - in tablets or ointment form.
- Ibuprofen is one of the most common medications that is easier to tolerate by the body than others.
- Indomethacin - attractive at an affordable price, relieves pain well, but it has many contraindications.
- Ketoprofen - in the form of tablets, injections, ointments, aerosols, gels, suppositories and even a preparation for applications.
- Movalis is less toxic to the gastrointestinal tract than many others, but is contraindicated in patients with diseases of the cardiovascular system.
- Nimesulide – copes with pain and inflammation, and also helps stop the destruction of joints.
- Etoricoxib requires strict adherence to the dosage, otherwise complications from the heart and blood vessels are possible.
There are a lot of drugs in the NSAID group: they must be prescribed by a doctor
Basics of Anti-Inflammatory Drug Treatment
The pronounced effect of antirheumatic drugs develops after one and a half to two months of regular use. Treatment with these drugs is usually very long-term (most often lifelong).
Glucocorticoids should be administered in the early morning - at 6:00 - 7:00 am. With this mode of administration, the maximum therapeutic effect of the drugs is observed and their side effects are reduced.
As an analgesic or antipyretic, non-steroidal anti-inflammatory drugs should be used for no more than one week (usually up to 5-6 days); as an anti-inflammatory drug (for example, for inflammation of joints or ligaments) - no more than two months.
What are the contraindications?
- Ulcerative lesions of the gastrointestinal tract in the acute stage.
- Severe renal and liver dysfunction.
- Individual intolerance to the main active ingredient and auxiliary ingredients.
- Pregnancy and lactation.
- Individual intolerance to drug components.
- Children under 2 years old.
Anti-inflammatory drugs should be prescribed with caution to people suffering from bronchial asthma, as well as people who have already experienced adverse reactions when taking medications. For patients with arterial hypertension or heart failure, NSAIDs are chosen that have the least effect on renal blood flow. Elderly people are prescribed the minimum effective doses of NSAIDs in short courses.
Features of treatment with anti-inflammatory drugs
Antirheumatic drugs and glucocorticosteroids, by suppressing the immune system, make the body more sensitive to infections; in addition, they can mask the symptoms of acute infectious diseases.
Taking antirheumatic drugs should not be stopped abruptly - this is dangerous due to a sharp exacerbation of the disease (withdrawal syndrome). Therefore, discontinuation of these drugs should be carried out by gradually reducing their dose over 10-14 days.
To reduce the negative effect on the stomach and reduce the risk of ulcers in the stomach while taking glucocorticosteroids and non-steroidal anti-inflammatory drugs, it is recommended to use drugs that protect the gastric mucosa (misoprostol, omeprazole).
Types of anti-inflammatory drugs
Modern medications cope with inflammation of any nature and have a long-lasting effect. They are often prescribed when pain needs to be relieved.
- Hormonal drugs . They have a much stronger effect than non-hormonal ones. The basis of such drugs is cortisol. They act on the principle of local immune suppression. And at the same time, such drugs have many more contraindications and side effects.
They are prescribed for severe skin allergies, rheumatoid arthritis, vascular inflammation, hepatitis, and inflammation of skeletal muscles.
- Combined means . These medications include combinations of several components. Thanks to this, the therapeutic effect is greatly increased.
- Nonsteroidal drugs . These drugs act selectively on types of cyclooxygenase, inhibiting their activity. COX is responsible for the creation of biologically active components. Due to the suppression of COX activity, the amount of these substances in tissues decreases and inflammation disappears.
Diagnosis
Before making preliminary conclusions and making a diagnosis, the gynecologist will collect an anamnesis. Diagnosis of inflammation of the appendages is valuable, but the doctor will prescribe treatment only after clarifying the degree of damage to the body and identifying the causative agent of the disease. Adnexitis is one of the diseases of the genital area that requires instrumental intervention for diagnosis.
First, the doctor conducts a clinical examination of the patient in a gynecological chair. The exact picture of the disease does not always become clear, so the gynecologist prescribes ultrasound diagnostics. The procedure will reveal changes in the genital organs, as well as confirm the presence of inflammation in the body. It is extremely rare for a specialist to prescribe an MRI. Typically, the diagnostic method is used when cancer is suspected.
A mandatory step in making a diagnosis is taking tests. They help determine the exact type of causative agent of the disease. The doctor prescribes:
- bioseeding;
- PCR;
- examination of a smear under a microscope.
The biomaterial is the patient’s vaginal secretions or blood. Rarely is an oral sample used for testing. A general blood test will confirm the presence of inflammation in the body, but will not determine the strain of pathogenic microorganisms.
Side effects during long-term treatment with high doses of GC
In conclusion, I would like to add that in the fight against chronic pain syndrome, which accompanies many diseases, steroid analgesics help indirectly and are only part of the therapy. It is important that the drug, dosage and duration of the course are selected by the attending physician in accordance with the results of examinations, indications, medical history and the individual characteristics of the patient’s body. It is not recommended to independently adjust the course of treatment to avoid side effects.
Anti-inflammatory therapy of acute respiratory diseases
Acute respiratory diseases (ARI) remain the most common reason for people seeking medical help. Children get sick more often, on average 4–6 times a year, and sometimes up to 8–12 [1]. However, in many cases, adolescents and adults are treated for mild and even moderate forms on their own, calling a doctor only when complications develop. As a result, the true incidence is difficult to estimate. Of course, a significant number of episodes of acute respiratory infections with a mild course can be successfully treated with the help of over-the-counter products and remain unaccounted for.
In addition to acute respiratory infections, when symptoms of intoxication are combined with rhinitis and pharyngitis, doctors often diagnose patients with acute respiratory viral infection (ARVI). However, in the absence of laboratory diagnostic results, it is not easy to differentiate viral and bacterial etiology, and in some cases it is impossible, especially in the first day from the onset of the disease or in case of atypical etiology (mycoplasma, chlamydial). Often there is one or another combination of viruses and bacteria. Therefore, for practice, the term ORZ remains the most convenient.
Many studies over the past decades have shown that in most cases, viruses are the etiological factor of acute respiratory infections [1–3]. Among them, parainfluenza viruses, influenza A and B, rhinoviruses, adenoviruses, respiratory syncytial viruses and herpes group viruses are often found. Metapneumovirus, bocavirus, coronaviruses, reoviruses, and enteroviruses are detected less frequently, which is largely due to the low prevalence of their laboratory diagnosis and the lack of awareness of their importance among doctors. Recently, it was shown that rotaviruses can also cause the development of acute respiratory infections symptoms even in the absence of vomiting and diarrhea [4]. Bacterial flora (Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, Moraxella catarrhalis and others) is detected much less frequently. Studies have shown that they can be detected in healthy individuals, but become a cause of disease in people with weakened immunity, more often in children of early and preschool age, the elderly and those suffering from severe chronic pathology. Almost as much as typical bacterial pathogens (about 10-15%), in the etiological structure of acute respiratory infections are atypical flora - Mycoplasma pneumoniae and Chlamydophila pneumoniae [5-8]. Of course, the contribution of one or another microorganism will vary from year to year depending on the territory, season and the population being examined. In many cases, a comprehensive laboratory examination does not allow determining the etiological factor. This may be due to a violation of the technique for collecting material for analysis, non-compliance with transportation conditions, lack of appropriate diagnostic reagents, an unknown variant or mutation of the pathogen.
The main clinical symptoms of acute respiratory infections caused by various infectious agents are the same: fever, rhinitis, pharyngitis, and sometimes tonsillitis, laryngitis and tracheitis are added [2, 5, 9]. Sinusitis, otitis, stomatitis, epiglottitis, bronchitis, pneumonia are considered complications. The frequency and severity of one or another manifestation of the disease depends on both the pathogen and the characteristics of the patient’s body.
The doctor should prescribe therapy immediately after the first examination of the patient, without waiting for the results of a laboratory examination. In most cases of outpatient practice, it does not seem absolutely necessary, with the exception of the diagnosis of influenza and streptococcal infections, since there are currently no drugs specifically acting against one pathogen other than anti-influenza drugs. During inpatient treatment of complications, severe and life-threatening forms, etiological diagnosis is necessary to assess the prognosis and select the most effective treatment regimen, taking into account the properties of the pathogen.
The impossibility of prescribing reliable etiotropic therapy primarily dictates the need to select active pathogenetic therapy. Of course, it reduces the severity of symptoms and speeds up recovery time both when treated with anti-flu drugs and when prescribing antibacterial agents. The key element in the pathogenesis of acute respiratory infections is the inflammatory syndrome. Due to it, swelling of the structures involved in the infectious process, excessive mucus production, impaired mucociliary clearance, and narrowing of the airway lumen develops. Inflammation is a protective reaction developed during evolution aimed at localizing and subsequent elimination of the pathogen. However, an excess of inflammatory components can lead to a significant deterioration of the condition, an increase in the duration of the disease, and sometimes to a gross dysfunction of the respiratory system and other organs. This can occur due to the individual hyperreactivity of the body itself, stimulation of α-adrenergic receptors by respiratory viruses, which is accompanied by an intensification of the secretion of viscous mucus, and the effect of the pathogen on H1 receptors, which causes an increase in the permeability of the vascular wall with the accumulation of secretions and tissue swelling [10]. The release of pro-inflammatory mediators promotes the migration of new cells into the lesion, the destruction of which releases new active substances that increase swelling and accumulation of mucus.
In modern living conditions, air pollution in combination with a high concentration of microorganisms in public places forms an almost constant reaction of the mucous membranes of the respiratory tract, the severity of which depends on the individual characteristics of the body. Natural reactions to contact with a pathogen are combined with previously formed ones, which leads to severe swelling, narrowing of the lumen, and intense secretion of viscous mucus. Obstructed outflow contributes to the development of complications: sinusitis, otitis, bronchitis, pneumonia. Against this background, the risk of developing life-threatening conditions increases: obstructive laryngitis and status asthmaticus.
Numerous studies have shown that reducing the activity of the inflammatory process has a beneficial effect on the course of acute respiratory infections: it reduces the severity of symptoms, alleviating the patient’s condition, shortens the duration of the disease, and prevents the development of complications [11]. Glucocorticosteroids have been used for many years as active anti-inflammatory drugs. However, their side effects occur quite often: increased blood pressure, increased symptoms of heart failure, hypokalemia with concomitant heart rhythm disturbances and convulsions, hyperglycemia, prolonged or recurrent infectious diseases, gastrointestinal lesions, obesity and many others. Numerous adverse events have sharply limited their frequency of use. Non-steroidal anti-inflammatory drugs are recommended more often, for acute respiratory infections - mainly as antipyretics and painkillers. Their suppressive effect on inflammation is known. However, an increase in the amount of leukotrienes due to a redistribution of arachidonic acid metabolic pathways often leads to damage to the gastrointestinal tract, bronchospasms and other side effects.
The search for drugs with an anti-inflammatory effect that are safe for use by patients of any age led to the emergence at the end of the last century of a new group of drugs - inhibitors of arachidonic acid metabolism, which are neither glucocorticosteroids nor non-steroidal anti-inflammatory drugs. The first such substance was fenspiride. The mechanism of its action is to reduce the influx of calcium into leukocytes, which activates phospholipase A2. As a result, the amount of produced arachidonic acid and its metabolites: prostaglandins, thromboxane, leukotrienes, is reduced, which leads to a decrease in the severity of edema at all levels of the respiratory tract. Its effectiveness was confirmed in animal experiments [12].
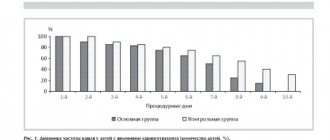
Since the appearance of fenspiride on the pharmaceutical market at the end of the last century, a large number of studies have been conducted on its effect on the course of acute respiratory infections in children and adults. The total number of participants was more than 6 thousand [13–16]. The results were largely similar. They showed that the drug acts on almost all symptoms of acute respiratory infections, reduces the duration of the disease by 2–3 days, and ensures recovery in 71% of children by the 7th day, and the rest by the 10th day. At the same time, in the comparison group, relief of symptoms by the end of the first week was observed in 50% of patients, and in the other half - during the 2nd week [13]. The drug has an effect against nasopharyngitis, laryngitis, tracheitis, bronchitis, sinusitis, and otitis [14, 15]. Prescribing such a drug turns out to be most beneficial in conditions where it is impossible to predict the dynamics of the development of the infectious-inflammatory process. At first, as a rule, you are worried about nasal congestion with certain discharge (manifestations of rhinitis), sore or sore throat, and coughing. Hyperemia is visually determined, sometimes - granularity and/or swelling of the posterior wall of the pharynx, which characterizes pharyngitis. Practicing doctors are well aware that with some infections (for example, parainfluenza) from the nasopharynx, symptoms quickly spread to the larynx, trachea and bronchi. Laryngitis develops with cough and hoarseness, tracheitis with a frequent, predominantly dry cough, and then bronchitis. In patients who are often ill or have chronic pathology of one or another part of the respiratory tract, the risk of spreading the infectious process increases sharply. Fenspiride prescribed for symptoms of nasopharyngitis will have an anti-inflammatory, anti-edematous and hypersecretion-suppressing effect in laryngitis, tracheitis, bronchitis, bronchiolitis, and pneumonia [14–16].
We observed 140 patients with acute respiratory infections, aged from birth to 90 years (of which 64 were children and adolescents, 76 adults), who received fenspiride in recommended age-specific dosages. The main indication for prescribing this drug was a cough that developed due to an inflammatory process in the nasopharynx (all 140 patients were diagnosed with acute nasopharyngitis). Many patients were also diagnosed with changes in the underlying parts of the respiratory tract: the larynx (acute laryngitis was noted in 25), trachea and bronchi (acute tracheitis in 8, acute bronchitis in 29, bronchiolitis in 6). At the same time, 54 patients at the time of fenspiride prescription had a combination of two or three clinical forms. Basic therapy in most cases consisted of irrigation of the nasopharynx with saline solutions or antiseptics (118 patients), antipyretics as needed. Antiviral therapy was used in 43 patients, antibacterial therapy in 38.
On the 3rd day after the start of treatment with fenspiride, 132 patients (94%) showed an improvement: the frequency of coughing and coughing attacks significantly decreased, especially during night sleep, the intensity of a sore throat and nasal discharge decreased. By the 7th day, recovery was noted in 103 patients (74%), by the 10th - in another 21. In 13 patients aged 36 to 90 years, improvement was noted by this time, but cough persisted, which was associated with exacerbation of chronic bronchitis in the absence of acute respiratory infections symptoms. By the 21st day, against the background of prolongation of fenspiride therapy, the exacerbation in this group of patients was stopped. In three patients under our supervision, the drug was changed due to the development of adverse events, possibly related to the prescribed treatment.
It should be noted that good results of therapy were noted by both patients and their parents in cases of observation of children of early and preschool age. This is confirmed by the fact that during subsequent episodes of acute respiratory infections, they insisted on prescribing fenspiride or began taking it on their own before being examined by a doctor.
Our results of observation of patients confirm previously published data on the effectiveness of fenspiride in various manifestations of acute respiratory infections, including against the background of chronic obstructive pulmonary disease [17]. When prescribed in a timely manner, it provides prevention of complications: bronchitis, bronchiolitis, pneumonia, sinusitis, otitis. In cases of starting treatment with existing symptoms of the development of an infectious process outside the nasopharynx, which often occurs with infection with parainfluenza, respiratory syncytial viruses, adenoviruses, metapneumovirus (frequent development of laryngitis, bronchiolitis, bronchitis, especially in children), the drug helps relieve symptoms and reduce recovery period. With the development of acute respiratory infections against the background of chronic changes in one or another part of the respiratory tract, fenspiride also has a therapeutic effect.
Studies have shown that the drug significantly reduces the intensity of a dry obsessive cough, promotes its transition to a wet one, and then accelerates its relief [13, 14]. At the same time, fenspiride, unlike glucocorticosteroids and non-steroidal anti-inflammatory drugs, exhibits side effects much less frequently. The drug is usually well tolerated: it does not have a negative effect on the gastrointestinal tract, blood pressure, glucose and potassium levels.
Of the 140 patients under our supervision, during treatment of acute respiratory infections with fenspiride, adverse events were noted in only three (2%): two (women 38 and 54 years old) had complaints of tachycardia, and one (child 11 years old) had complaints of tachycardia. for nausea. It should be noted that palpitations appeared against the background of changes, according to electrocardiograms (complete block of the left bundle branch in one patient and Wolff–Parkinson–White syndrome in the second), and in the presence of a diagnosis of chronic gastroduodenitis in the child. This indicates a possible exacerbation of the existing chronic pathology in connection with acute respiratory infections, and the connection with taking the drug seems doubtful. Other studies have also shown that the incidence of adverse events when taking fenspiride is insignificant: 2.4%, according to N. A. Geppe et al. [13].
Thus, fenspiride is recommended for the treatment of acute respiratory infections in patients of any age. Its anti-inflammatory effect helps relieve the main symptoms, shorten the period of the disease and prevent complications, including in patients with underlying chronic pathology of the respiratory system.
Literature
- Pediatrics. National leadership. Brief edition / Ed. Baranova A. A. M.: GEOTAR-Media 2015. 768 p.
- Trukhan D.I., Mazurova A.L., Rechapova L.A. Acute respiratory viral infections: current issues of diagnosis, prevention and treatment in the practice of a general practitioner // Therapeutic archive. 2016; 11: 76–82.
- Usenko D.V., Gorelova E.A., Kanner E.V. Rational approach to the treatment of ARVI and influenza in the clinical practice of a pediatrician // Russian Medical Journal. 2015; 3: 174–177.
- Ploskireva A. A., Gorelov A. V. Is a respiratory form of rotavirus infection possible? // Infectious diseases. 2016; 14 (3): 22–31.
- Lvov N.I., Likhopoenko V.P. Acute respiratory diseases. Guide to infectious diseases: in 2 books. 4th ed., St. Petersburg: Foliant, 2011; 2(III): 7–122.
- Blasi F. Atypical pathogens and respiratory tract infections // Eur. Respira. J. 2004; 24: 171–181.
- Pricipi N., Esposito S., Blasi F., Allegra L. Role of Mycoplasma pneumoniae and Chlamydia pneumoniae in children with community-acquired lower respiratory tract infections // Clin. Infect. Dis. 2001; 32:1281–1289.
- Savenkova M. S. Chlamydial and mycoplasma infections in pediatric practice // Consilium Medicum (Appendix 1). Pediatrics. 2005; 1: 10–17.
- Kupchenko A. N., Ponezheva Zh. B. Modern principles of diagnosis and treatment of ARVI // Archives of Internal Medicine. 2016; 1 (27): 6–12.
- Kozlov V.S. The role of inflammation in the pathogenesis of respiratory diseases // Consilium medicum. 2003; 5 (10): 213–225.
- Spichak T.V. Place of anti-inflammatory therapy for acute respiratory diseases in children // Pediatrics. 2012, 91(5): 67–73.
- Evrard Y., Kato G., Bodinier MC, Chapelean B. Fenspiridide and inflammation in experimental pharmacology // Eur. Respira. Rev. 1991; 1 (2): 93–100.
- Geppe N. A. Program “Elf”: effectiveness and safety of using Erespal for acute respiratory diseases in children // Consilium Medicum (Appendix 1). Pediatrics. 2005; 1:29–32.
- Korovina N. A., Ovsyannikova E. M., Dalilova I. E. Complex therapy of obstructive bronchitis with the use of Erespal (fenspiride) in young children // Klin. pharmacology and therapy. 2001; 5:1–4.
- Samsygina G. A., Fitilev S. B., Levin A. M. Results of a multicenter study of the effectiveness of fenspiride hydrochloride (Erespal) in the treatment of acute respiratory infection in young children // Pediatrics. 2002; 2: 81–85.
- Soroka N. D., Korshunova E. V., Gomozova S. P., Vlasova T., Kotelnikova V. N. Experience with the use of fenspiride in the early rehabilitation period for pneumonia in children // Pulmonology. 2010; 1:93–98.
- Grigorieva N. Yu., Mayorova M. V. Anti-inflammatory therapy of respiratory diseases with fenspiride // Russian Medical Journal. 2015; 4: 216–219.
T. A. Ruzhentsova, Doctor of Medical Sciences
FBUN TsNIIE Rospotrebnadzor, Moscow
Contact Information