Let us pay attention to a problem that is relevant for almost 80% of Russians. Let's figure out how to correct a malocclusion in an adult, because straightening teeth is quite possible not only in childhood. We need to look at the effective ways in which orthodontists make their patients' smiles beautiful and healthy.
We will try to pay maximum attention to the features and differences of the methods so that, if necessary, you can choose the most suitable one for yourself. And be prepared for the fact that the final decision will still have to be made together with the doctor. Because the type of intervention and program of procedures depend on the nature of the pathology, and only a specialist can accurately diagnose its degree and adequately assess the chances of success.
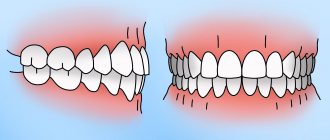
Types of malocclusion
- open - the teeth either do not close at all, or a significant gap is visible between many of them;
- deep – the exact opposite situation, that is, there is an overlap of approximately half the length;
- mesial – the lower jaw, compared to the upper, is moved forward;
- distal – the problem is the opposite of the previous one;
- cross - the right and left sides protrude unevenly, the cutting edges close together.
Other anomalies include:
- diastema - a gap between the front pair of incisors;
- three - noticeable gaps between “neighbors” along the gum;
- twisting - creeping of sixes, fours, fives onto each other;
- transposition - eruption in the wrong places, right up to the palate.
Any of them is not just inconvenient or bad from an aesthetic point of view, but can also provoke the emergence and development of a number of diseases. It develops against the background of genetic abnormalities and heredity, appears due to injuries and loss of bone tissue.
Methods for restoring chewing teeth. Modified approach
V. V. Shcherbakov , dentist, Royal-Dent aesthetic dentistry clinic (Moscow)
The main goal of restoration of chewing teeth is, first of all, functional rehabilitation. Functionality, in turn, is determined by the anatomical correctness and accuracy of the manufactured structure. The convex and relief chewing surface forms multiple point contacts with antagonist teeth, evenly distributing the occlusal load. The contact points should be small in area, ensuring rapid opening of the teeth during excursion movements.
Wide and flat occlusal surfaces are more likely to remain in contact during mandibular movements. This creates friction, leading to more pronounced wear of teeth and restorations and a decrease in chewing efficiency. Hardly anyone would dispute the need to accurately reproduce chewing morphology when carrying out restoration. However, achieving this goal for the vast majority of doctors is fraught with significant difficulties. One of the most common problems is that the doctor, after painstaking and lengthy modeling of the chewing surface, has to mercilessly cut off all the tubercles and fissures with a bur at the stage of integrating the tooth into the occlusion.
The approaches that will be discussed in this article are designed to greatly facilitate the work of doctors
All the beauty that a specialist recreates ultimately turns into a shapeless, unaesthetic and low-functional “cake”. The dental literature describes a large number of various techniques to avoid such difficulties (compass method, orientation to adjacent teeth, occlusal compass, all kinds of schematizations, simplified construction algorithms, etc.). However, all these solutions provide only approximate results. The approaches that will be discussed in this article are designed to greatly facilitate the work of doctors and will allow the production of high-precision restorations. The main idea taken as the basis for this approach is that, depending on the degree of tooth decay, correspondingly different methodological variations of restoration are used. It should, however, be noted that these techniques are focused on working with vital teeth, that is, in conditions favorable for the formation of a strong adhesive connection. According to the degree of destruction, three conditional classes can be distinguished (the classification was developed by the author of the article).
Method of restoring teeth of the 1st class of decay
A typical representative of class 1 is fissure caries, which is quite common. This pathology is very unpredictable, and often the volume of the lesion turns out to be much greater than the expected depth. The fissure form of caries, as a rule, is characterized by almost complete preservation of the chewing morphology, and no matter how high the skill of the restorer, we still will not be able to recreate the chewing surface better than it was. Therefore, it would be quite reasonable to copy the preserved anatomy and transfer it to a future restoration. This can be achieved using the occlusal key technique. The main difference between this approach and the traditional restoration option is that before the preparation, a key (small impression) is removed from the chewing surface, which could subsequently be used to press down a portion of the composite to give it the original tooth shape. The most suitable material for making a key is hard bite silicones for bite registration. They have sufficient hardness to push through the smallest details of the chewing surface, and at the same time practically do not stick to the composite.
Clinical case
Figure 1 shows the initial situation. Classic fissure caries of teeth 16 and 17. As in most similar cases, the carious process is completely asymptomatic.
Rice. 1
After isolating the working field (Fig. 2) and mechanically removing plaque from the surface of the teeth, the key is removed with bite-silicone, taking into account the dimensions of the clamp (Fig. 3).
Rice. 2
Rice. 3
The appearance of the occlusal key is shown in Figure 4.
Rice. 4
Next, preparation and adhesive preparation are carried out using the XP Bond™ system based on tert-butanol (Fig. 5).
Rice. 5
After restoration and polymerization of the dentinal layer (Ceram•X™ duo+), shades of the base and surface enamel (Esthet•X® HD A2 and AE) with a total thickness of 1.5-2 mm were added one after another, carefully adapted to the surface with approximate contours marked without subsequent curing (Fig. 6).
Rice. 6
Now comes the turn of the occlusal key (Fig. 7).
Rice. 7
To prevent possible gluing, apply a small amount of adhesive to the silicone surface. The key is placed on the tooth and pressed slowly. After the silicone print is in place, you need to slowly remove it with light rocking movements. You should not rush and try to remove the key with one jerk: this will lead to deformation of the composite material. If done correctly, the portion of uncured enamel composite should take the exact shape of the original occlusal surface (Figure 8).
Rice. 8
Excess filling material is easily removed with a brush. If any deformation occurs, the key can be reinstalled. Next, polymerization is carried out for 30-40 seconds, taking into account the thickness of the composite layer (Fig. 9).
Rice. 9
After this, if desired, you can reproduce the characteristics using composite paints. View after finishing and polishing (Fig. 10).
Rice. 10
Occlusal correction is usually minimal or absent. View of the restorations after two days (Fig. 11).
Rice. eleven
It should be noted that an important condition for successful restoration using the occlusal silicone key technique is the use of composite materials that have a sufficiently dense consistency and are capable of retaining the shape transferred by the silicone key. In this regard, a very good option is the Esthet•X® HD composite, which, in addition to excellent chromatic and mechanical characteristics, also has the required degree of density and perfectly holds any shape.
Method of restoring teeth of the 2nd class of decay
Among the clinical cases of this category, deep carious cavities and failed fillings are most common. The main feature of the second class is that with fairly high destruction - up to 50% of the chewing surface - the main outlines of tubercles, ridges, parts of the ridges, etc. are still preserved. Having such landmarks at our disposal, we can easily continue the external contours of the preserved occlusal elements and get a chewing surface very close to the original. For this, the traditional method of layer-by-layer restoration is used, without any changes. The only addition that could help make the restoration more comfortable is the use of modeling tools in a specific sequence.
Algorithm for restoring the chewing surface. Three Tools Concept
Figure 12 shows the initial situation.
Rice. 12
Figures 13-15 show the layer-by-layer introduction of material into the cavity: a layer of dentin, a layer of chromatic enamel (the composite is distributed throughout the cavity without polymerization), a layer of surface enamel.
Rice. 13
Rice. 14
Rice. 15
To adapt the material, it is convenient to use a brush slightly moistened with adhesive (Fig. 16).
Rice. 16
Next, tool No. 1 is used - a large plugger for preliminary marking of all chewing elements (Fig. 17).
Rice. 17
They also outline the lines of future fissures and remove excess material. Modeling continues with tool No. 2 - a small plugger, which reproduces all the main forms, brings out additional ridges, side ridges, secondary recesses, and also emphasizes fissures of the first order (Fig. 18).
Rice. 18
At this stage, the excess composite is finally removed. In some cases, a small brush with lubricant can be used to make anatomical transitions smoother. The last tool (No. 3) is a sharp probe for creating the thinnest elements and emphasizing fissures (Fig. 19).
Rice. 19
After this, polymerization of the composite material is carried out (Fig. 20).
Rice. 20
As a final element, the pigmentation of the fissures can be reproduced with composite paints using a thin endodontic file (Fig. 21-23).
Rice. 21
Rice. 22
Rice. 23
Clinical case
In (Fig. 24) the situation before treatment. An old, failing filling with obvious secondary changes in the surrounding tissue.
Rice. 24
The working field is isolated (Fig. 25) and the carious cavity is prepared (Fig. 26).
Rice. 25
Rice. 26
The quality of treatment is controlled by a caries detector. The deepest areas of the cavity were also stained, but in this case it was not the demineralized tissue that was stained, but the tertiary reaction dentin. Due to the fact that this type of dentin is formed compensatory in response to the action of irritants and is not structurally complete, has cellular inclusions and voids, it is also susceptible to indication by a caries detector. This dentinal bridge is usually the last stable barrier to the pulp chamber and should not be removed. Next, the cavity is sandblasted (Fig. 27) and adhesively prepared with the 5th generation XP Bond™ system (Fig. 28).
Rice. 27
Rice. 28
After thoroughly drying the adhesive before polymerizing it, a very thin layer of low modulus SDR™ composite was applied to the dentin and then co-polymerized. The purpose of this technique is to stabilize the hybrid zone, as well as to prevent the formation of an oxygen-inhibited layer in the adhesive interface.
Part of the cavity is filled with SDR™ composite (Fig. 29).
Rice. 29
It has a high ability to self-adapt, very low polymerization stress and optical characteristics similar to dentin. A portion of Ceram•X™ duo+ D3 composite is applied on top of the SDR™ material to imitate dentin (Fig. 30), then a layer of Esthet•X® HD YE surface enamel (Fig. 32) and a layer of Esthet•X® HD A3 chromatic enamel (Fig. 31).
Rice. thirty
Rice. 31
Rice. 32
The composite spreads over the surface, but does not polymerize. Figure 33 is a view after an instrumental simulation carried out in strict accordance with the three-instrument concept described above.
Rice. 33
Next, the characteristics were reproduced (Fig. 34, 35).
Rice. 34
Rice. 35
Figures 36, 37 show the view after occlusal integration, finishing and polishing.
Rice. 36
Rice. 37
It should, however, be remembered that in order to successfully perform a restoration using the traditional technique, the doctor certainly needs to have some experience and developed skills in anatomical modeling. The most effective way to learn to accurately reproduce the chewing surface is constant practical training.
You need to draw teeth, sculpt them from plasticine, grind them from plaster, model them from wax, reproduce them in the mouth with a composite, etc. All this must be done, guided by the general principles of shaping and knowledge of the myotopography of anatomical elements. Gradually, a sense of form will develop, the ability to “read” characteristic anatomical details, some dependencies will be revealed, and in the end a complete understanding of the entire process of reconstruction of the occlusal surface will come.
Method of restoring teeth of the 3rd class of decay
This category of defects includes large-scale carious lesions, voluminous old fillings, uncomplicated chips of tubercles, walls and any other pathologies characterized by a large deficiency of hard tissues. Such teeth are on the border of indications for direct methods of restoration, and in cases where the destruction of the crown reaches a level of more than 50% of the volume, indirect restorative structures such as composite or ceramic inlays, overlays or crowns are indicated. The biggest challenge in reproducing occlusal morphology in clinical cases in this category is the lack of sufficient landmarks. Under such conditions, we cannot find the required shape and determine the correct spatial position of each anatomical element. In the dental laboratory, such problems are solved with the help of preliminary wax modeling of the teeth in a correctly adjusted articulator. This technique is based on exactly the same principle: before starting tooth restoration, preliminary modeling with a composite is carried out in the mouth directly on top of old fillings and pathologically changed areas. The doctor reproduces the morphology of the tooth as he sees fit, and then checks the occlusal relationship, removing excess with a bur. Thus, all major corrections are carried out at the beginning of work on a preliminary composite model, and not on the finished restoration.
Clinical case
Figure 38 shows the initial situation.
Rice. 38
Deep carious cavity of tooth 26 with significant destruction of the palatodistal, palatomedial cusps, as well as the accessory cusp of Carabelli. The demineralization process, however, is stabilized, the bottom of the cavity is solid, and is practically not stained with a caries detector. Upon completion of the modeling, the necessary occlusal corrections are made (Fig. 40).
Rice. 40
As a result of all articulation tests, a shape is created that can be transferred to the final restoration in the future using a silicone key. Before preparing the cavity, a preliminary composite modeling of the chewing surface is carried out, reproducing all the missing anatomical elements (Fig. 39).
Rice. 39
The procedure is performed before anesthesia is administered and without a rubber dam. Figure 41 shows the process of removing the key using hard silicone.
Rice. 41
Excess impression material is cut off taking into account the dimensions of the future clamp. The view of the occlusal key is shown in Figure 42, the view after preparation is shown in Figure 43.
Rice. 42
Rice. 43
Next, adhesive preparation of the cavity was carried out with the XP Bond™ system (Fig. 44), and the dentinal layer was reproduced with Ceram•X™ duo+ D3 material (Fig. 45).
Rice. 44
Rice. 45
Then, one after the other, without polymerization, the base and surface layers of enamel (Esthet•X® HD A2 and AE) are added and adapted (Fig. 46).
Rice. 46
Due to the fact that after preliminary modeling we receive only an approximate occlusal blank without anatomical nuances, we will need to finish them with thin instruments on the enamel layer after pressing the composite with a key (Fig. 48).
Rice. 48
This must be done carefully so as not to displace the position of the main masticatory hillocks. If serious deformation of the material has occurred, you can try to press the tooth again with a silicone template. Pressing the uncured composite with a silicone key is shown in Figure 47, the view after clarifying the chewing morphology is in Figure 49.
Rice. 47
Rice. 49
The characteristics are reproduced (Fig. 50).
Rice. 50
Figure 51 shows a view of the restoration after occlusal integration, grinding and polishing, and Figure 52 shows a view after three days.
Rice. 51
Rice. 52
Conclusion
These methodological approaches make it possible to obtain the most accurate results of restorative treatment, even when restoring severely damaged teeth. Optimal composite materials also have significant potential to interact with the presented techniques.
Signs of correct bite
Normally, the jaws make close contact when closing. In this case, the upper teeth cover the lower ones by about a third, so that the palatal tubercles of the former touch the incisors of the latter. There are no gaps between them both when the mouth is closed and during chewing. The facial proportions are symmetrical.
Also among the characteristic features:
- absence of speech defects;
- no clicking or other similar discomfort in the joint;
- ease of biting food.
And vice versa, if problems are observed in any of the points just listed, this is an alarm bell and a reason to consult an orthodontist, and immediately, without waiting for the situation to worsen.
Massage for teeth straightening
Massage of the gums and palate is one of the most painless methods of comprehensive correction of dental anomalies. It is carried out while performing hygienic procedures for caring for the oral cavity. Massage in a circular motion along the gums using a medium-hard toothbrush.
As a result of such manipulations, local blood circulation will improve, pain will go away when wearing orthodontic structures, and the alignment process itself will go faster. Regular massage will strengthen your gums and prevent loosening of your teeth.
Why you need to straighten your teeth
Please note that the question is not whether it is worth correcting the bite - it simply needs to be done, and for several reasons:
- To avoid increased abrasion, caries, removal - when everything is normal, all incisors are evenly used when chewing, and in case of disturbances, some work more, others less; The former lose enamel faster and chip, the latter are less resistant to bacteria.
- To prevent diseases of the temporomandibular joints as a result of their mutual displacement. This pathology is also unpleasant due to bruxism, muscle spasms, clicking and crunching.
- To protect the gums, tongue and inner cheeks from injury caused by out-turned or tilted incisors.
- In order to grind food well during eating, not to create additional stress on the gastrointestinal tract and not to provoke problems with stool, enterocolitis, gastritis.
- To prevent problems with ENT organs and breathing, eliminate the source of bacterial accumulation and not give a single chance to sore throat, sinusitis, and otitis media.
People who have experienced complexes about their chin and then decided to have surgery or wear braces can tell a lot about whether to correct their bite. After medical help, they are much more willing to show their smile when communicating.
Correction of teeth shape
One of the most common reasons why patients turn to a dental esthetician is to correct the shape of their teeth. It should be noted that when we say “correction of the shape of teeth,” in 90% of cases we mean: correction of the front teeth, or more precisely, the teeth in the smile zone. Teeth may have an unaesthetic shape from birth, or they may acquire it throughout life. In the first case, specialists most often encounter gum hyperplasia (excessive growth of soft tissue) or disproportionate development of teeth. In the second case, the shape of the teeth is disrupted for two reasons: either due to increased abrasion, or as a result of injury, when the enamel or even a piece of the tooth (for example, a corner of the cutting edge) often chips. A special case is frantic lovers of gnawing seeds; this bad habit in severe cases provokes horseshoe-shaped abrasion of the front incisors.
In the case of gum hyperplasia, when soft tissues excessively cover the teeth, making them visually smaller and shorter, the problem is solved using laser gingivoplasty, when the “excess” mucous membrane is removed, exposing the tooth surface. In cases with increased tooth wear, the patient is prescribed, first of all, orthodontic treatment to correct occlusion, because malocclusion is the most common cause of this problem, and then teeth are corrected - extensions using composite materials or ceramic crowns. The same applies to correcting chips and cracks; in such cases, dental restoration or installation of ceramic veneers are also often used.
Diagnosis of anomalies
There are obvious cases, such as a pronounced diastema or torsion, you can notice them yourself when standing in front of a mirror. But there are also minor disorders that are no less dangerous to health, and only a specialized doctor can identify them.
Usually, hidden defects are easily recognized by a dentist - when he conducts a preventive examination, removes plaque or places a filling. Then he describes the problem and gives a referral to an orthodontist, who will determine how to straighten the jaw, bite, and a couple of adjacent teeth. To do this, a specialist will conduct a thorough examination of the patient’s mouth with a computed tomography or x-ray.
The anomaly can also occur during life, for example, after injury. Therefore, it makes sense to visit a doctor regularly, every six months, so that he either confirms that everything is in order, or promptly notices unwanted changes, which are easier to stop at the initial stage.
Trainers
Trainers are a special device for straightening teeth, resembling a mouthguard. This method is as effective as aligners, but more affordable.
The advantages of this method:
- Can be used to straighten children's teeth;
- It will not only help straighten your teeth, but also relieve problems such as pacifier or finger sucking, improper breathing or tongue positioning;
- Helps straighten teeth for children and adults;
- Does not require constant use, overnight is enough;
- You can buy it yourself;
- With the help of trainers, you can correct problems with diction, malocclusion and abnormal tooth growth;
- Do not interfere with eating or talking;
- Do not require special maintenance;
- Low price.
Disadvantages of this method:
- Long treatment period - from a year or longer;
- At first wearing it causes discomfort;
- There is a possibility of the mouthguard falling out during night wear.
To completely correct crooked teeth, you need to go through three stages of treatment. At the first stage, soft blue trays are used. They promote habituation and prepare the dentition for harder structures. At the last stage, the patient uses retainers (a device for preventing the curvature of teeth), which is worn only at night and is a metal case that is fixed in the palate of the mouth and remains practically invisible.
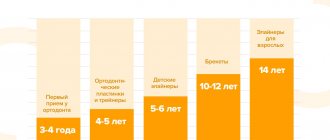
Up to what age is correction possible?
For many decades it was believed that the impact would be successful only in childhood, and during primary and secondary school, and not later. But with the development of orthodontics, things have changed. Today, achieving a healthy smile is not difficult at any stage of life - the main thing is that the person himself wants it, so that he is ready to patiently follow a number of medical prescriptions.
What is the problem with correcting bites in adults?
A child's jaw is in the process of growing, so it is more flexible and easier to change. At the age of 15, this is generally easiest to do: the incisors move relatively easily, they are fixed more securely - you have to wear braces for a year, no longer.
For a mature person, a similar procedure will take from 2 to 3 years, because his bone tissue is already formed. It is impossible to expand the space between the teeth, to move them apart; there is simply no free space. In some cases, you even have to remove, say, completely healthy eights.
Another nuance is that, say, at the age of 30, you will also need to consolidate the achieved result, and it will take a long time - from 20 to 40 months. Sometimes people wear retainer structures for almost the rest of their lives. This is explained by the fact that the incisors have already become “accustomed” to their positions and tend to take them again after the braces are removed.
Aligners (aligners)
An aligner is a mouth guard made of silicone or soft plastic that exactly follows the contours of the teeth and works like a brace system, albeit slowly but effectively straightening the teeth. Despite the proven effectiveness of aligners, they are not used so often, mainly to correct bites.
The advantages of this method:
- Almost invisible on the teeth;
- Easy to remove while eating or brushing your teeth;
- Does not cause discomfort;
- There are no restrictions on food when wearing a mouth guard;
- Does not cause pain when wearing;
- You can treat “oral” problems while wearing a mouth guard;
- Do not cause allergies;
- Along with straightening, you can also whiten your teeth;
- Has no contraindications.
Disadvantages of this method:
- Not effective for complex problems;
- High price;
- Before eating, food must be removed prematurely and stored properly;
- Long production time (mouthguards are often delivered from abroad).
In order to comprehensively straighten crooked teeth using a mouth guard, you need to go through several stages. First, the dentist takes impressions of the teeth and creates an electronic model. The same layout is necessary at intermediate stages of treatment, as well as at the end of the procedure. For the entire stage of treatment, you need several drops, which should be changed after 2-3 weeks, as prescribed by the doctor.
The patient should wear the mouth guard at least 22 hours a day and remove it only to eat and brush teeth. The duration of treatment is from 6 to 8 months, and in case of prophylaxis.
Disadvantages of composite restoration
Each technique, therapeutic or aesthetic, has its drawbacks. For direct composite dental restoration this is:
- The resulting ideal color of the composite lasts approximately 3-4 years.
- The service life of new fillings is not long enough compared to porcelain material.
- Increased risk of formation of secondary carious lesions in comparison with ceramic structures.
- If the volume of restoration is very large, then this affects the strength. Ceramics are considered more reliable.
There is also a risk of choosing the wrong shade of the composite, which will differ from real enamel. However, the high qualifications and extensive experience of our dentists exclude such an unpleasant situation.
How is restoration done with composites?
Stages of artistic correction in modern dental clinics:
- Removal of hard deposits and soft plaque;
- Selecting the appropriate color of the composite material;
- Local anesthesia;
- Removal of affected tissue and previously installed fillings;
- Creation of a dry working field;
- Treatment of the area with antiseptics;
- Creation of a crown by layer-by-layer application of filling material.
The last stage of correction is to adjust the crown to the specific patient. First, the shape is changed so that the patient does not feel discomfort when biting or chewing. The filling is then polished to a state identical to the enamel.
Why do teeth grow at random?
Malocclusions are often caused by heredity. If parents have certain defects in the dental system, we can guess what dental problems their child will face. However, some systemic diseases, injuries, and improper oral care in childhood also lead to crooked teeth.
The main reasons why adult teeth are positioned incorrectly:
1.Underdevelopment of the dental system
Oddly enough, this is a problem of the accelerated development of civilization and the inability of the human body to adapt so quickly to a new environment. We began to eat freeze-dried food, which does not contribute to the development of the dental system. Genetically, the number of teeth remains the same, but the jaws do not receive the proper load and remain underdeveloped. As a result, teeth grow crowded and become crooked.
2.Premature tooth loss
If a baby tooth is removed before its due date, neighboring teeth tend to take its place, and the dentition is formed incorrectly. Further correction requires considerable time and financial costs. However, the problem concerns not only milk teeth, but also permanent teeth. Injuries sustained in adulthood can cause serious abnormalities. The long-term absence of one or more dental units leads to irreversible consequences: neighboring teeth are displaced, the bite is disrupted.
3. Problematic wisdom teeth
In addition to the fact that the eights themselves can grow crookedly, they contribute to the crowding of the remaining teeth. There is not enough space in the dentition for their full growth; from the moment they erupt, they harm neighboring teeth.
If you are embarrassed about your smile, contact an orthodontist - the problem can be solved.
Classification of dental gaps
Diastemas
– these are gaps of any size between the front central incisors. Tremae are spaces between any other teeth in the upper or lower jaw. Gaps between the lower front incisors are uncommon, but gaps between the upper central teeth can be seen several times more often. In many cases, the presence of a diastema of this kind provokes serious psychological discomfort, interfering with the harmonious socialization of patients.
Depending on what type of teeth are – baby or permanent – a distinction is made between false and true gaps between them. False dental gaps are observed in children - such defects go away on their own along with the change of teeth. True gaps form between permanent teeth and can only be removed with specialized help from a dentist. Doctors advise starting to correct such defects immediately after they occur, since then it will require much less time and effort.
Where to get dental restoration done in Moscow?
Since dental restoration is a real art that requires the highest professionalism and considerable talent from the dentist, it is necessary to carefully choose a clinic and a specialist.
Dentistry "PROFI-Dent" is:
- an integrated approach to each clinical case;
- a team of true masters of their craft;
- the latest technical equipment;
- advanced materials and restoration technologies;
- ideal results in the shortest possible time.
The cost of aesthetic restoration work in our clinic will surprise you with its democratic nature, and the result will exceed your expectations!
Braces price for bite correction
| Consultation with an orthodontist | FOR FREE |
| Alginate impression | 1000 rub. |
| Diagnostic model calculation | 2500 rub. |
| Making a diagnostic model (2 pcs.) | 2500 rub. |
| Observation during the treatment phase | 1000 rub. |
| Treatment of malocclusions (bite alignment) | from 70,000 rub. |
| Fixation of one bracket on NO MIX material | 1800 rub. |
| Fitting and applying the arc | 500 rub. |
| Tying the arch to one bracket | 400 rub. |
| Fixation of elastic traction (1 link) | 500 rub. |
| Setting the spring | 800 rub. |
| Making a wire retainer and fixing it | 5000 rub. |
| Making a retention splint | 5000 rub. |
| Manufacturing of an orthodontic plate with 2 clasps from imported plastic | 11000 rub. |
| Manufacturing of 2-jaw apparatus, regulators, bionators and various modifications of functional apparatus | 16,000 rub. |
| Positioner | 15,000 rub. |
| Cementation of the orthodontic ring | 850 rub. |
| Removing one bracket | 500 rub. |
| Removing one ligature | 300 rub. |
| Clinical correction of the device | 1000 rub. |
| Repair of orthodontic apparatus (in the laboratory) | 2500 rub. |
| Activation of the orthodontic appliance | 1000 rub. |
| Fitting and fixing the palatal clasp | 1500 rub. |
| Correction of teeth with the INVISALIGN system (excluding the technical part) | from 70,000 rub. |
| Photo recording (1 photo) | 250 rub. |
| Surgery to install an orthodontic implant | 11000 rub. |
| Taking a one-step two-layer impression (A-silicone) | 3250 rub. |
How to straighten teeth in adults?
More and more people today agree that it is necessary to correct uneven teeth. “How to straighten teeth in adults aged 30 or more” is one of the most common queries on the Internet on the topic of dentistry. This is a positive trend, which means that the level of public awareness and desire to change their smile is growing every year. Today, there are several methods that allow you to straighten teeth in adults of almost any age. Let's talk about everyone in order.
How to choose a good doctor
With a large number of offers of dental services in Moscow, it is difficult to make a choice where and in what way to straighten teeth without braces for adult patients. The reputation of the clinic, the equipment used, the quality of the materials used, and the qualifications of the doctors are of great importance.
First of all, pay attention to the following factors:
- extensive practical experience, working with similar clinical cases, certificates;
- conducting a thorough preliminary examination and competent recommendations;
- availability of modern computer technologies for treatment planning;
- positive reviews online and in the professional environment, recommendations from other patients;
- working with high-quality materials and manufacturers of orthodontic products with an impeccable reputation.
In most cases, orthodontic services are quite expensive. Saving on treatment costs can adversely affect the final result and lead to complications. At the Federal Scientific and Clinical Center of the Federal Medical and Biological Agency of Russia, you can straighten your teeth under optimal conditions, without compromising the quality of work.
Gap between teeth: what should be done?
If you have a very small diastema, then a visit to the dental clinic can wait. However, even a small gap should be regularly monitored by a doctor, since tooth gaps tend to grow over time. However, if the diastema is significant, it is better to visit the dentist as soon as possible. This defect can contribute to the development of caries, malocclusion, gum disease, etc. Various methods have been developed for correcting diastemas. Typically, the doctor carries out treatment on an individual basis and selects a method that will be most effective for a particular patient. The technique is chosen based on the reasons for the appearance of a gap between the teeth, the size and degree of development of the dental gap, and the wishes of the person himself.