Chewing function and the muscles responsible for it
Without these muscles, we would have to be fed intravenously.
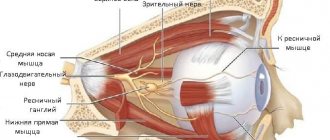
Their well-coordinated teamwork allows us to dig into our favorite burger and enjoy a cold milkshake with appetite. The four main paired muscles of mastication - the masseter proper, medial pterygoid, lateral pterygoid and temporal - are attached to the skull and lower jaw. They are responsible for movements of the temporomandibular joint .
The buccal and mylohyoid muscles play an auxiliary role in the process of eating and drinking.
Muscles of Mastication : These powerful muscles lift your lower jaw so you can close your mouth and chew food.
One of the strongest facial muscles, the masseter muscles are thick, flat, and rectangular in shape and are attached to the lower jaw and cheek bones on either side of the face.
Medial pterygoid muscles : these muscles have three functions.
Being also located on both sides of the head, they work as follows:
- With the simultaneous contraction of both muscles, the lower jaw moves forward.
- Contraction of one medial pterygoid muscle leads to movement of the jaw in the opposite direction - this is how we move the jaw left and right.
- Thanks to the simultaneous work of the medial pterygoid, masticatory and temporal muscles, we are able to close our mouth and bite.
These muscles are attached to the pterygoid processes of the sphenoid bones of the skull and the inner surface of the angles of the lower jaw.
Lateral pterygoid muscles: the work of these muscles is no less important - they are responsible for opening the mouth, and after you bite off a piece of, for example, pie, they help chew it.
These short, wing-like muscles are located above the medial pterygoid muscles on either side of the head.
Temporalis muscles: The temporalis muscles, which look like large fans, are located, as you might guess, at the temples and help close the mouth.
Cheek muscles: we don’t bite our cheeks when chewing food This is due to the fact that the cheek muscles keep them at a safe distance from the teeth.
You can understand where the cheek muscle is located by touching with your fingers the depression on the inside of the cheek between the upper and lower jaws.
The cheek muscles have three functions, two of which are not related to mastication:
- Helps you avoid biting your cheeks while eating.
- They control the movement of air flow in the oral cavity when whistling, inhaling and exhaling, which is necessary for normalizing breathing and playing wind musical instruments.
- Together with other muscles, they help us smile.
Mylohyoid muscles : swallowing movements play an important role not only in nutrition, but also in the act of articulate speech. When you swallow, a pair of mylohyoid muscles help raise the floor of your mouth, making this action easier.
Muscles depressing the lower jaw: - mylohyoid, - geniohyoid, - anterior belly of the digastric muscle. Places of attachment: - Mylohyoid - flat, participates in the formation of the muscular base - the diaphragm of the oral cavity. It starts from the line of the same name of the lower jaw and is attached by posterior bundles to the anterior surface of the body of the hyoid bone, and the main part of the muscle fibers meets the fibers of the muscle of the same name on the opposite side, forming a fibrous suture. Function: Raises the hyoid bone, and when the hyoid bone is fixed, lowers the lower jaw. - Geniohyoid - located above the mylohyoid muscle. It starts from the mental spine of the lower jaw and attaches to the body of the hyoid bone. Function: pulls the hyoid bone up and forward, and when supported by the hyoid bone, lowers the lower jaw. - Anterior belly of the digastric muscle - the anterior belly begins from the digastric fossa of the mandible. It is connected by a tendon to the second belly and is attached to the body and greater horn of the hyoid bone through a dense fused loop. Function: lowers the lower jaw, pulls it back. With a fixed lower jaw, it raises the hyoid bone. Muscles that lift the mandible: - The masticatory muscle itself; - Temporalis muscle; - Medial pterygoid. Places of attachment: - The masticatory itself is rectangular, starts from the lower edge of the zygomatic arch, attaches to the lateral surface of the coronoid process of the mandible, as well as to the masticatory tuberosity of the mandible. Function: raises the lower jaw. — The temporal jaw is wide, fan-shaped, and occupies the area of the same name on the lateral surface of the skull. It starts from the temporal surface of the large wing of the sphenoid bone, the squama of the temporal bone. Attached to the apex and medial surface of the coronoid process of the mandible. Function: raises the lower jaw, the anterior fascicles pull the jaw upward to the front, the posterior fascicles pull it back. - Medial pterygoid - starts from the pterygoid fossa of the same process of the sphenoid bone, attaches to the pterygoid tuberosity on the inner surface of the angle of the lower jaw. Function: with unilateral contraction, it moves the jaw in the opposite direction; with bilateral contraction, it moves the jaw forward and lifts it. Muscles that protract the mandible: Paired lateral pterygoid muscle. With their synchronous contraction, the lower jaw moves forward; with unilateral contraction of the muscle, the lower jaw moves in the opposite direction, thus the muscles of the third group provide anterior and lateral movement of the lower jaw. Place of attachment: Located in the inferotemporal fossa. It starts from the infratemporal crest and the maxillary surface of the greater wing of the sphenoid bone, from the lateral plate of the pterygoid process of the same bone: it is attached to the articular capsule of the TMJ, the articular disc, and the anterior surface of the neck of the lower jaw. Function: with unilateral contraction, it shifts the lower jaw to the opposite side, with bilateral contraction, it pushes it forward.You might be interested in:
- Bite
- Central occlusion
- Movements of the lower jaw.
- Strength of masticatory muscles
- Functions of chewing
We recommend reading:
- Dentition
- Mucous membrane.
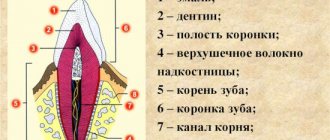
- Temporomandibular joint (ellipsoidal incongruent, paired, complex). Consists of: - glenoid fossa; - articular head; - articular bu...
"> Temporomandibular joint
- Solid sky
- The upper jaw is a paired bone. Each half has a body and 4 processes: - frontal; - zygomatic; - palatal; - alveolar...
">Structure of the upper jaw
Medical Internet conferences
Distal occlusion of the dentition ranks first among pathologies of the dental system. It accounts for 12.4 to 65% of cases of all occlusion anomalies in adolescents and adults. The number of adult patients with this pathology seeking orthodontic care is constantly growing.
Various deformations of the dentition, with distal occlusion, are always accompanied by functional overload of the teeth, dysfunction of the temporomandibular joint and affect the functional state of the muscles of the maxillofacial area.
Functional disorders with distal occlusion of the dentition are detected in 63% - 89% of the examined patients.
In patients with distal occlusion of the dentition, increased tension in the buccal, facial and mental muscles and weakening of the orbicularis oris muscle were revealed.
These functional changes in the muscular system are observed when distal occlusion is formed. Meanwhile, as the cause of the development of distal occlusion, in addition to genetic features of development, the role of disturbances in the activity of the muscular system, leading to secondary deformations in bone structures, is considered. The fact is that the facial muscles can have a dual effect on jaw growth. First, bone formation at muscle insertions depends on muscle activity; secondly, muscles are an important part of the entire tissue base, the growth of which usually moves the jaws.
Most often, changes in the muscles of the maxillofacial area are caused by long-term, incorrectly performed function. Violation of the distribution of chewing pressure leads to structural changes in the supporting apparatus, deformation of the dentition, and occlusion. Moreover, in some muscle groups there is hyperfunction, and in others hypofunction, which causes significant changes in both those and others in the form of compensatory-adaptive deformation, characterized by a restructuring of the fiber composition (the ratio of phasic and tonic muscle fibers), metabolism and contractile properties. It is well known that the adaptive result of increased work is hypertrophy of muscle fibers, while hypofunction is accompanied by a decrease in muscle mass - atrophy.
It is also believed that functional disorders in the form of disturbances in myodynamic balance in the maxillofacial region play a significant role in the formation of distal occlusion of the dentition. Functional disorders are one of the most important reasons for the development of dental anomalies and deformities.
The purpose of the study is to improve the diagnosis of muscle disorders in patients with distal occlusion of the dentition.
Material and methods of the study: 70 people of both sexes aged 15-18 years were examined and 2 age groups were identified: with physiological occlusion (FO) (35 people) and distal occlusion of the dentition (DO) (35 patients).
The type of occlusion of the dentition was determined when they were closed in the usual position of the lower jaw. In patients with DO, during a clinical examination, a violation of the closure of the first molars and the frontal group of teeth was observed (the sagittal incisive gap was 3.0 ± 0.5 mm).
Anthropometric and X-ray (TRG in lateral projection) studies were performed.
Using the method of surface electromyography, biopotentials (BP) were studied in the group of muscles that lift the mandible - the anterior parts of the right and left temporal (Vp and Vl), the right and left muscles of mastication (Zh and Zl), in the muscles that depress the mandible - the right and left suprahyoid muscles ( NPp and NPl) and in the cervical muscles, balancing the position of the head on the spinal column ensuring the position of the lower jaw at rest - the right and left sternocleidomastoid muscles (Sp and GL). Registration was carried out using a computerized electromyograph “Electromyograph BKN” manufactured by Biotronic (Italy).
The bioelectric signal from the muscle, through electrodes, was transmitted to a computer, where it was amplified, purified, and visualized on the monitor screen in real time using the KEY-NET computer program according to specified programs (functional tests).
During the electromyographic study, the following functional tests were used:
Test 1: State of relative rest of the lower jaw (dentitions are not closed, lips slightly touching).
Test 2: State of physiological occlusion of the dentition (primary contact of pairs of antagonist teeth, closure of teeth without load).
An analysis of the amplitude values of biopotentials (BP) was carried out, where two main digital systems for calculating average amplitude indicators of BP are used - ARV and RMS.
In addition to recording and analyzing the average amplitudes of BP of muscles calculated in the RMS and ARV systems, the following indicators were analyzed: total BP of the studied muscles of the right side; average biopotential of the studied muscles on the right (SBP) (sum of BP indicators of the right temporal, masticatory, suprahyoid and sternocleidomastoid muscles divided by 4) or on the left (sum of BP indicators of the right temporal, masticatory, suprahyoid and sternocleidomastoid muscles divided by 4); total biopotential (GBP) (µV) - the sum of all BP indicators of the muscles of the right and left sides; percentage expression of the BP of each studied muscle in the RBP (according to ARV (%) and RMS (%); indicator of the maximum amplitude of biopotentials (MAX) (μV).
Research results:
When studying the biopotentials of the muscles of the maxillofacial area in both digital calculation systems - ARV and RMS, no statistically significant differences were found between the indicators of identical muscles. The RMS and ARV systems have equal capabilities in assessing the functional state of the muscles of the maxillofacial area. Therefore, the RMS calculation system was randomly selected for further research.
1. Persons with physiological occlusion of the dentition
1.1. Relative rest of the lower jaw .
In a state of relative rest, the values of biopotential (BP) indicators of the temporal and masticatory muscles of the right side are higher than those of the left. In the group of muscles depressing the mandible and in the sternocleidomastoid muscles, the digital values on the left side were slightly higher than on the right. There is a “cross” asymmetry in the BP parameters of the maxillofacial muscles (Table 1).
It should be noted that 90% of the examined patients had a predominantly right-sided type of chewing.
However, when comparing the indicator of the own biopotentials of all muscles of the right side (Vp+Zhl+NPp+GKp) (2.3±0.5 μV) with the indicator of the own biopotentials of all muscles of the left side (Vl+Jl+NPl+GKl) (2.0 ±0.2 µV) no significant differences were found, which indicates the myodynamic balance of the muscles of the maxillofacial area.
Expressed as a percentage, the biopotentials of the muscles that lift the mandible on the right side are greater than on the left. In the muscles depressing the mandible and in the sternocleidomastoid muscles, a significant predominance of the muscles of the left side over the right was observed.
The percentages of the levator and depressor mandibular muscles were also compared. A larger percentage of the total bioelectrical activity (TBA) is contributed by the muscles that elevate the lower jaw - 58%, than the muscles that lower it - 16%. 26% were the sternocleidomastoid muscles (Table 1).
1.2. Physiological occlusion of the dentition (habitual closure).
With the usual closure of the dentition, in the muscles that elevate the mandible, the BP of the muscles on the right side predominates, and in the muscles that depress the mandible, the BP on the left side predominates.
In the sternocleidomastoid muscles, BP indices on the left are 1.4 times higher than those on the right (Table 2).
When comparing the BP indices of all the studied muscles during closure of the dentition with the BP indices of identical muscles with relative rest of the lower jaw, no significant differences were revealed in any of them.
Expressed as a percentage, in relation to the total biopotential (TBP) of the studied muscles, the BP of the right temporal and masticatory muscles is significantly greater than that of the left ones. In the muscles depressing the mandible and in the sternocleidomastoid muscles, the percentage of PD on the left is greater than on the right.
The percentage of BP of the mandibular levator muscles on the right side is higher than on the left. The percentage of PD of the right and left temporal and masticatory muscles was 60%. The percentage of PD of the muscles depressing the mandible on the right side is lower than on the left. The percentage of PD of these muscles was 16% (Table 2).
When comparing the indicated indicators when closing the dentition with the corresponding indicators during physiological occlusion, no statistically significant differences were identified for any of them.
Differences in the maximum amplitude of the BP in the temporalis, masseter, suprahyoid and sternocleidomastoid muscles were statistically insignificant between the right and left sides.
2. Patients with distal occlusion of the dentition.
2.1. Relative rest of the lower jaw.
It was found that the BP of the temporal and masticatory, suprahyoid and sternocleidomastoid muscles turned out to be absolutely equal on the right and left.
BP indices in patients with distal occlusion had higher values than BP indices of similar muscles in individuals with physiological occlusion, with the exception of the right masseter muscle.
The average biopotential (ABP) of the studied muscles on the right and left sides was 2 times higher than these indicators in individuals with physiological occlusion (Table 3).
There were no differences between the percentage of BP of the right and left side in any muscle group, while in individuals with physiological occlusion, a significantly higher percentage of BA was found in the muscles of the levator mandible on the right, and in the depressor muscles on the left.
2.1. Closing of the dentition in patients with distal occlusion.
The values of BP of the muscles that raise and lower the lower jaw when closing the dentition on the right and left did not differ significantly and were significantly higher, in contrast to the indicators recorded in individuals with physiological occlusion, where similar indicators were significantly different from each other. There is an increase in the indicators of BP of the temporal muscles, on the right and on the left, compared with those of the masticatory muscles by 2.6 times and 2.1 times, respectively.
When analyzing the average biopotential (ABP) of the muscles of the right and left sides, values were established that did not differ significantly from each other, but were 1.7 times and 1.8 times higher than the values of the SBP of muscles in persons with physiological occlusion of the dentition (Table 4 ).
Analysis of the percentage of BP showed that there are no differences in the muscles of the same name on the right and left sides. Meanwhile, when comparing these indicators with the indicators in individuals with physiological occlusion and with the indicators of patients with distal occlusion at rest, a significant increase in the percentage of PD of the temporal muscles was established.
Discussion
When conducting surface electromyography in persons 15-18 years old with physiological occlusion of the dentition in a state of relative rest of the lower jaw, the values of the biopotentials of the temporal and masticatory muscles on the right side are higher than on the left. The biopotential values of the suprahyoid and sternocleidomastoid muscles on the left side are higher than on the right. The average biopotential of the muscles on the right side is equal to the average biopotential of the muscles on the left side. The total biopotential (TBP) of all muscles studied is 16.7±0.4 μV. In persons with physiological occlusion of the dentition, the indicators of the biopotentials of the muscles of the maxillofacial region, when the dentitions are closed, do not differ from the indicators of the biopotentials of the muscles under study with relative rest of the lower jaw.
In patients aged 15-18 years with distal occlusion of the dentition, the muscles of the maxillofacial region at rest are in a state of increased bioelectrical activity, which indicates their hypertonicity. The greatest increase in bioelectrical activity develops in the temporal (1.8 times in the right and 2.9 times in the left) and suprahyoid muscles (3.6 times in the right and 2.4 times in the left) compared with the indicators recorded in persons with physiological occlusion. The values of the total biopotential (SBP) of the muscles on the right and left sides and the total biopotential (TBP) of the muscles of the maxillofacial region exceed these indicators in persons with physiological occlusion by 2 times. During the initial contact of pairs of antagonist teeth, the work of the muscles is discoordinated, as indicated by a significant predominance of the biopotential values of the temporal muscles over the masticatory muscles (2.0 times on the right and 1.6 times on the left).
Conclusion
The results of the conducted studies deepen knowledge on the functional state of the muscles of the maxillofacial area in individuals with physiological and distal occlusion of the dentition.
The data obtained make it possible to effectively use, for diagnostic purposes, computerized electromyographs with analysis of indicators of bioelectrical activity of the muscles of the maxillofacial area in one of the systems for calculating average values of biopotentials - RMS or ARV.