Author of the article:
Soldatova Lyudmila Nikolaevna
Candidate of Medical Sciences, Professor of the Department of Clinical Dentistry of the St. Petersburg Medical and Social Institute, Chief Physician of the Alfa-Dent Dental Clinic, St. Petersburg
Before talking about the treatment of pulpitis with unformed roots, you need to understand what unformed roots are.
After the eruption of baby teeth, their roots have an uncovered apex for several years, which is why they are called unformed.
Features of the treatment of pulpitis on teeth with unformed roots
Treatment of pulpitis on such teeth has its own characteristics. Due to the fact that it is impossible to completely treat the entire length of the tooth roots and extract the pulp, traditional devital and vital methods for treating teeth with immature roots are not suitable. Therefore, pediatric dentists use biological treatment methods or the amputation method.
Conservative treatment
It should be noted that biological (conservative) treatment is a rather complex process that has a number of contraindications. The main principle of treatment is maintaining absolute sterility. It is very important to carry out high-quality antiseptic and aseptic processing.
During the biological treatment of pulpitis, the dentist, under anesthesia, removes not only plaque, but also all affected and dead dental tissue, prepares the tooth cavity and applies medicine to the exposed nerve (or to the bottom of the carious cavity). As a rule, this medicinal paste contains calcium hydroxide. After all pain symptoms disappear after a few days, a permanent filling can be installed. The main thing is that as a result of this treatment, the tooth retains its vitality and strength, and the pulp provides nutrients to its tissue.
Amputation method for treating teeth with immature roots
Due to the complexity of biological treatment and the existing contraindications to this method, this method is used infrequently by dentists. And most doctors prefer amputation, during which the doctor removes the infected pulp from the pulp chamber using a vital or non-vital method.
- The devital method using arsenic compounds is not used in every clinic today. Some dental offices use phenol-formalin to necrotize the pulp. To do this, a swab moistened with this solution is applied to the tooth cavity for 4-5 days.
- Most often, pediatric dentists treat pulpitis using the vital method, without the use of arsenic. To do this, doctors use not only local anesthesia, but also various antibacterial drugs, calcium-containing drugs and remineralizing agents. During this method, the pediatric dentist, after taking care of anesthesia, excises the upper part of the pulp and applies a special preparation. Thanks to this method, it is possible to preserve the root pulp, which means that in the future the dental roots will continue their normal formation.
Alternative
Prevention of pulpitis is careful adherence to hygiene rules. Use Asepta toothpastes, which effectively strengthen tooth enamel and prevent the growth of bacteria in the oral cavity.
Principles of treatment for incomplete root formation
The goal of therapy is to eliminate inflammation and complete root formation in the tooth. Periodontitis contributes to the death of the growth zone, so the dentist must direct efforts to form a dense barrier in the area of the unformed apex.
During the first visit, the following manipulations are performed:
- necrotomy, formation of a carious cavity;
- opening of the dental cavity;
- removal of putride masses, taking into account the length of the root, which is previously determined on an x-ray;
- removal under anesthesia of granulations grown into the canal;
- complete instrumental treatment of the canal - removal of infected predentin from the walls with an H-file with a safe apex, copious rinsing with antiseptics, but without excessive pressure, so as not to accidentally push the solution beyond the unformed apex;
- drying the canal;
- administration of a medicine with an antiseptic effect, for example in the form of a paste;
- isolation of the dental cavity with a sealed bandage made of filling material for the purpose of temporary obturation of the carious cavity.
Depending on the period of action of the medicine, the following visit is prescribed, during which the following manipulations are performed:
- remove the bandage and the contents of the canal;
- wash it with an antiseptic solution;
- filled with a paste based on calcium hydroxide;
- isolate the cavity with a sealed dressing, for example glass ionomer cement.
Sometimes long-term obturation with calcium hydroxide paste is performed on the first visit. To do this, the following conditions must be met:
- the channel initially contains no products of putride decomposition;
- there is no gangrenous smell in it;
- there is no fistula on the mucosa;
- the child does not complain of pain or discomfort;
- the patient is somatically healthy;
- There are all conditions for channel processing in one visit.
After about a month, the contents of the canal are replaced with fresh paste. Further tactics, along with planned treatment of dental caries in children, involve replacing calcium hydroxide-containing paste in the canal every 3-6 months. Before this, it is necessary to take an x-ray of the state of root formation. After the formation of a dense apical barrier, the presence of which will be confirmed by x-rays and probing, permanent obturation can be performed.
Clinical researches
“Results of clinical use of the Asepta series of products: already at the first control examination (after 1-2 days) of using the Asepta line of products, there is a decrease in complaints of discomfort, but bleeding persists when brushing teeth. On the 7th day, complaints of gum bleeding persisted in 4 patients. Upon examination, a decrease in hyperemia and swelling of the gums was noted, but bleeding persisted upon probing. After the final application of the gel with propolis, normalization of clinical manifestations was revealed, which is manifested by the absence of bleeding during brushing and probing.”
Sources:
- The effectiveness of the use of Asept “adhesive balm” and Asept “gel with propolis” in the treatment of chronic generalized periodontitis and gingivitis in the acute stage (Municipal Dental Clinic No. 4, Bryansk, Kaminskaya T. M. Head of the therapeutic department Kaminskaya Tatyana Mikhailovna MUZ City Dental Clinic No. 4, Bryansk
- Study of the clinical effectiveness of treatment and prophylactic agents of the Asepta line in the treatment of inflammatory periodontal diseases (A.I. Grudyanov, I.Yu. Aleksandrovskaya, V.Yu. Korzunina) A.I. GRUDYANOV, Doctor of Medical Sciences, Prof., Head of Department I.Yu. ALEXANDROVSKAYA, Ph.D. V.Yu. KORZUNINA, asp. Department of Periodontology, Central Research Institute of Dentistry and Maxillofacial Surgery, Rosmedtekhnologii, Moscow
- The role of anti-inflammatory rinse in the treatment of periodontal diseases (L.Yu. Orekhova, A.A. Leontyev, S.B. Ulitovsky) L.Yu. OREKHOVA, Doctor of Medical Sciences, Prof., Head of Department; A.A. LEONTIEV, dentist; S.B. ULITOVSKY, Doctor of Medical Sciences, Prof. Department of Therapeutic Dentistry of St. Petersburg State Medical University named after. acad. I. P. Pavlova
- Report on the determination/confirmation of the preventive properties of personal oral hygiene products “ASEPTA PLUS” Remineralization doctor-researcher A.A. Leontyev, head Department of Preventive Dentistry, Doctor of Medical Sciences, Professor S.B. Ulitovsky First St. Petersburg State Medical University named after. acad. I.P. Pavlova, Department of Preventive Dentistry
- Clinical studies of antisensitive toothpaste “Asepta Sensitive” (A.A. Leontyev, O.V. Kalinina, S.B. Ulitovsky) A.A. LEONTIEV, dentist O.V. KALININA, dentist S.B. ULITOVSKY, Doctor of Medical Sciences, Prof. Department of Therapeutic Dentistry, St. Petersburg State Medical University named after. acad. I.P. Pavlova
Treatment of periodontitis in baby teeth
Treatment of periodontitis in a baby tooth is aimed at removing the infection in the tooth and beyond, located in the ligament that holds the tooth. Most often, treatment of periodontitis of a baby tooth does not lead to successful preservation of the tooth, so a surgical treatment method is quite appropriate in this case.
Child's complaints. With periodontitis, complaints may include food getting stuck in the tooth, pain when biting on the tooth, constant pain that gets worse when biting, or there may be no complaints. It all depends on the degree of damage to the tooth.
What can parents see in their baby's mouth? A large cavity in the tooth, a severely damaged tooth, the absence of the crown part of the tooth, inflammation on the gums of a round shape of different sizes, colors, and sometimes diffuse inflammation of the gums. Purulent contents may also be released from the gums. The tooth may be mobile.
Treatment method. Conservative methods of treating periodontitis do not always achieve complete elimination of the source of infection, so there is a need for surgical intervention, ending with tooth extraction.
Recommendations. To avoid early tooth extraction and prevent dental anomalies, visit your dentist, but at least 3-4 times a year.
Complications
A slight aching pain after treatment is a normal reaction of the body. Normally, it lasts no more than a day. If the pain increases, swelling occurs, or the child’s general condition worsens, go to the doctor.
Perhaps the reason is individual intolerance to antiseptic drugs, which caused irritation of the periodontal tissues. In this case, physiotherapy is performed.
If the x-ray shows that the root filling was installed incorrectly, repeated mechanical and medicinal treatment of the canals is performed. This will neutralize and prevent secondary inflammation.
Stages and process of surgical treatment
Surgical treatment is used when gentle therapy does not relieve inflammation. Other indications for surgical intervention include obstruction of the root canals or granuloma (purulent sac).
To treat permanent teeth, root apex resection is performed:
- The canal is filled with a quick-hardening material.
- Under local anesthesia, an incision is made in the gums in the area of projection of the tooth root.
- The area of bone is cut out, and the affected root tip is cut off.
- Then necrotic (dead) tissue and purulent exudate are scraped out.
- The cavity is filled with an antibacterial drug and a bone preparation.
- The wound is stitched up.
- In some cases, drainage is installed for a day.
This is a complex, time-consuming operation that lasts about 40 minutes. Therefore, you should consult with your doctor about using general anesthesia so that your child can safely endure the procedure.
Baby teeth that cannot be saved are removed without any preliminary manipulation.
Pulpitis in children classification
The tactics of its treatment and prognosis depend on what type of disease it is. Therefore, doctors always carry out differential diagnosis between them.
Classification of pulpitis according to the type of disease
Based on the speed of development and time of existence of the pathology, two types of pulpitis are distinguished: acute and chronic. The first is less common. It is characterized by rapid development and severe pain in the area of the affected tooth, which radiates into the jaw. It often occurs in response to a mechanical stimulus, and sometimes spontaneously. At the same time, children cannot explain or even understand exactly where it hurts. But appetite and sleep noticeably deteriorate: the child is uncomfortable eating, and at night the unpleasant sensations intensify (a clear sign of pulpitis in the child).
Chronic pulpitis is more common. Sometimes it appears even against the background of shallow caries. The child may not experience severe pain. Because of the fear of going to the doctor, children often do not admit the presence of discomfort. At this time, the disease progresses and complications form. It is especially important to pay attention to the child’s appetite after illness. Decreased immunity provokes exacerbation of pulpitis. In this case, the pain intensifies during chewing, which is why children may refuse to eat.
Classification of pulpitis according to the nature of the pathological process
When considering pulpitis as a disease, it is important what pathological process accompanies it. The set of measures necessary to treat the disease depends on this.
Types of pulpitis according to the nature of the pathological process
- Fibrous pulpitis - the connective tissue of the pulp grows and extends beyond the carious cavity. The child's pain occurs after eating and lasts for several hours. In the absence of adequate treatment, pulpitis enters the chronic stage.
- Hypertrophic pulpitis is rare in children. Characteristic signs: completely destroyed crown of teeth, absence of pain. The pulp bleeds during probing.
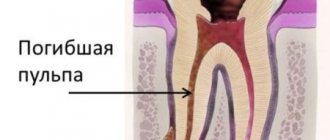
- Gangrenous pulpitis - the tooth begins to darken as the soft tissues die. The pulp disintegrates, which causes a putrid odor from the oral cavity. The pathology is often accompanied by the appearance of a purulent fistula on the gum. Since the pulp is dead, there is no pain.
In children, the development from fibrinous to gangrenous pulpitis occurs in just a few weeks. Therefore, it is important to pay attention to the child’s behavior (crying at night, refusing to eat) and immediately seek help from a dental clinic.
(stages of development of pulpitis)