All tissues of the oral cavity, both teeth and gums, are interconnected and naturally have a complex structure. Gums, just like teeth, require careful and thorough care. Periodontology is a separate science in dentistry that deals with the study of gum disease. Inflammation from the teeth can spread to periodontal tissue, and vice versa. Therefore, it is so important to maintain careful hygiene of the entire oral cavity and promptly treat any dental diseases.
Gum structure
The periodontium consists of a complex of tissues that form the entire periodontal space.
- Periodontium is a complex of fibers that hold the dental unit in the socket. The periodontium is located between the cementum and the alveolar wall. Nerve fibers, lymphatic vessels, veins and arteries are also located here, which together are responsible for the proper metabolism of the tooth.
- The gums are the outer part of the entire complex. The gums are the first to bear the brunt of harmful microorganisms that enter the oral cavity.
- The alveolar process is a bone plate that has a spongy structure and serves as a bed for the dental unit.
- Cement is the outer covering and protection of the tooth root.
- Enamel covers the crown of the tooth and is the hardest element of the entire complex.
- The pulp is the main source of metabolism in the tooth. Consists of blood vessels and nerve endings.
- Dentin is a substance located around the pulp and consisting mainly of mineral components.
Local factors:
Local factors include, first of all, dental plaque, which is a consequence of improper and untimely oral hygiene. It is a conglomerate of food debris and the bacteria that live in them.
Figure 3. Plaque under a microscope
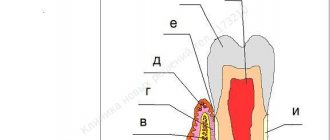
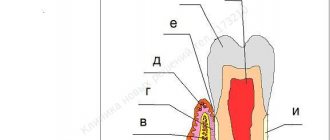
At first, the plaque is soft and can be easily removed with a toothbrush, but over time, bacteria firmly bind to the tooth enamel and the plaque gradually turns into tartar (1), which constantly injures the gums (2) and is a constant source of infection of the tissues surrounding it ( 3-6).
Figure 4. Local causes of periodontal disease development
In addition to dental plaque, local factors also include overload of periodontal tissues, insufficient chewing of food, and underload of certain groups of teeth.
Periodontal functions
In a healthy state, the periodontium performs a number of functions assigned to it:
- Support. The main function is due to which the tooth is held between bone plates.
- Shock-absorbing function. Correctly distributes pressure over the entire dentition.
- Trophic. A function responsible for nutrition and ensuring metabolism of the tissue complex.
- A protective function that helps create a barrier against the effects of bacteria.
- Reflex – affects the correct distribution of the chewing load.
- The plastic function is responsible for the elasticity of periodontal tissues.
What are the possible complications?
Improper teething, accompanied by pericoronitis without treatment, can lead to the following serious complications:
- Formation of necrotic ulcers along the gingival margin. Subsequently, necrosis can spread to other tissues of the oral cavity;
- Damage to healthy neighboring teeth;
- Phlegmon of the perimaxillary spaces;
- Periostitis, which easily spreads to nearby areas;
- Osteomyelitis;
- Abscess formation.
Any of these pathologies can become life-threatening, so treatment of inflammation of the mucous membrane must be timely.
Treatment of pericoronitis is not difficult. A timely visit to the dentist and diagnostics will allow you to immediately carry out the correct treatment. For example, if a tooth initially erupts incorrectly, then removing it at the very beginning of the process will avoid further discomfort.
If for one reason or another it was not possible to visit a doctor on time, then you should come for a consultation when the first signs of inflammation appear. The purulent form is much more difficult to treat and causes more inconvenience. In addition, pus is the main cause of complications.
The post Treatment of pericoronitis appeared first on.
]]>
Periodontal diseases
Reasons why gum disease occurs:
- soft and hard plaque on teeth;
- anomalies in the location of dental units;
- poor-quality prosthetics or treatment;
- genetic predisposition;
- reduced immunity;
- diseases of internal organs;
- hormonal imbalances in the body;
- constant stress;
- various bad habits;
- Irregular oral care.
In contrast to the large number of causes influencing the development of periodontal diseases, there are not so many diseases themselves:
- Gingivitis is the initial stage of gum inflammation.
- Periodontitis is an inflammatory process in the gums, gradually spreading to the alveolar processes of the jaw.
- Periodontal disease is a fairly severe form of the disease, characterized by exposure of the roots of the teeth.
- Periodontoma is the formation of tumors in soft tissues.
Blood supply to the periodontium –
The sources of blood supply to the periodontium are the superior and inferior alveolar arteries. In turn, smaller “dental arteries” branch off from them, which already penetrate the apical openings at the apexes of the roots of the teeth. Before penetrating the apical foramen, its alveolar and periodontal branches are separated from the dental artery. The bone wall of the alveoli throughout its entire length is penetrated by a system of perforated canaliculi, through which smaller arterioles penetrate from the alveolar branch of the dental artery to the periodontium.
Periodontal blood supply diagram –
The vascular network of periodontal tissues of adjacent teeth is combined into a single system, which allows for collateral blood flow. An important point is that periodontal vessels can be connected to intrapulpal vessels - through additional openings on the lateral surface of the tooth root. These may be ways for the infection to spread.
The lymphatic system is formed by capillaries that blindly begin in the intercellular substance of periodontal tissue, and is rather poorly developed. From the periodontium of the teeth of the upper jaw, the outflow of lymph occurs into the parotid lymph nodes, and from the teeth of the lower jaw - into the submandibular and sublingual lymph nodes. This is what explains the increase in certain groups of lymph nodes, for example, during exacerbations of chronic periodontitis.
Innervation of the periodontium –
It is carried out from the side of the trigeminal nerve, the afferent and efferent fibers of which form a plexus in the periodontal tissues. The endings of these fibers are pain receptors and mechanoreceptors. In most teeth, the maximum concentration of receptors is concentrated in the area of the root apices, but in the periodontium of the incisors, the receptors are evenly distributed throughout the periodontium. Sympathetic nerve fibers responsible for regulating blood flow are also found in the periodontium.
Treatment
Treatment of major periodontal diseases is as follows:
- removing all plaque and then polishing the teeth;
- treatment of existing carious formations;
- carrying out high-quality prosthetics, if necessary;
- splinting of the dentition (also carried out if necessary);
- treatment of existing common diseases;
- taking vitamins or medications;
- Regular cleaning of the oral cavity not only at home, but also in the dental office.
In the most difficult situations, in addition to the listed treatment, surgical intervention may be necessary.
General factors:
These are diseases of the body that contribute to the development of periodontal diseases. These primarily include:
- atherosclerotic vascular lesions (as a result of poor nutrition, increased cholesterol levels or hereditary predisposition);
- deficiency of vitamins C, B, A, E (poor nutrition, spring-autumn vitamin deficiencies);
- decreased body resistance to infections (most often respiratory);
- endocrine diseases (diabetes mellitus, parafunctions of the thyroid and parathyroid glands);
- diseases of the gastrointestinal tract (peptic ulcer, gastroesophageal reflux disease);
- blood diseases (anemia, pathology of the blood coagulation system).
What it is
Periodontium is periodontal tissue, the main function of which is to hold the tooth in the alveolus. All periodontal tissues are interconnected, so any changes in the functioning of one or another element inevitably affect the functioning of other elements. The periodontal structure includes periodontium, gums, alveolar processes and cementum. Some dental scientists also include tooth enamel, dentin and pulp in its composition.
The term “periodontium” appeared in dentistry a little over a hundred years ago and has since firmly taken its place in modern dentistry, although in Russia the term “took root” a little later, around the mid-30s of the last century. of periodontology deals with a thorough study of the periodontium, its main functions, structure, and possible diseases .
Gingivitis
Acute catarrhal gingivitis is an inflammatory process with a predominance of exudation. This disease is characterized by complaints of pain, itching, bleeding gums, and refusal to eat. Upon examination, hyperemia and swelling of the papillae, gingival margin, and sometimes the alveolar gum are determined, which leads to an increase in size and a change in the shape of the gingival papillae (not sharp, but rounded). When the alveolar gum is involved, its granularity (symptom of lemon peel), characteristic of healthy gums, disappears. Bleeding gums are detected when you touch them slightly. This form of gingivitis is observed relatively rarely, mainly during teething, as a result of acute trauma (mechanical, chemical, thermal), in acute childhood infectious diseases, and also as a manifestation of allergies, a symptom of acute herpetic stomatitis.
Chronic catarrhal gingivitis is the most common periodontal pathology in children. There may be no complaints; sometimes children notice bleeding gums when brushing their teeth. Upon examination, congestive hyperemia, pastosity, bleeding of the papillae and gingival margin are determined. The marginal gum is thickened like a roller (stretches like a rubber balloon), the surface becomes shiny. The granularity of the alveolar gum disappears.
With catarrhal gingivitis (both acute and chronic), with significant swelling of the gums, a gingival pocket, that is, a false periodontal pocket, can occur. The radiograph shows no changes in the alveolar bone.
Hypertrophic gingivitis is a chronic inflammatory process characterized by an increase in gingival papillae and marginal gums due to the proliferation of fibrous connective tissue and the basal layer of the epithelium. Most often, hypertrophic gingivitis is observed with close position of the teeth, open bite, small vestibule of the oral cavity, short frenulum of the lips, with improper orthodontic treatment, as well as during puberty (in girls with a late onset of menstruation or a long menstrual cycle, when the effect of estrogens predominates) , when taking antiepileptic drugs and blood diseases.
Hypertrophic gingivitis, caused by local factors (crowding of teeth, dental anomalies), is limited in nature, located mainly in the frontal area. Hypertrophic gingivitis, caused by endogenous causes (endocrine pathology, gastrointestinal diseases, etc.), is generalized, characterized by rapid development, a tendency to relapse and resistance to local treatment.
There are inflammatory (granulating) and fibrous forms of hypertrophic gingivitis. The inflammatory form is characterized by: hyperplasia of the gingival papillae, which are covered with granulations; their hyperemia with pronounced cyanosis and swelling; loose tissue and severe bleeding; pain on palpation; thickening of the gingival margin, its separation from the necks of the teeth, chronic catarrhal inflammation of the alveolar gum. False periodontal pockets are identified due to swelling and hyperplasia of the gums. There is a deposition of plaque and tartar. Hypertrophied marginal gum covers one or another part of the tooth crowns.
In the fibrous form, the gingival papillae are enlarged, dense, pale, do not bleed, and are painless.
According to the intensity of productive inflammation, there are 3 degrees of hypertrophic gingivitis:
— 1st degree — hypertrophy of gingival papillae;
— 2nd degree — hypertrophy of the gingival papillae and marginal gums;
— 3rd degree — hypertrophy of the marginal and alveolar gums.
Desquamative gingivitis is clinically characterized by swelling of the marginal gum, sometimes extending to the attached gum, pronounced hyperemia, severe bleeding and pain. A feature of this form of gingivitis is the constant desquamation of the surface layers of the gum epithelium, not only marginal, but also alveolar, as a result of which almost the entire mucous membrane becomes eroded and easily vulnerable. May occur against the background of hypertrophic gingivitis. Children complain of pain when brushing their teeth and eating, the presence of blood in saliva, the specific smell and taste of blood.
Desquamative gingivitis in children develops rarely, mainly during puberty (in girls, usually during a short menstrual cycle, when the action of progesterone predominates).