According to antiplagiat.ru, the uniqueness of the text as of October 16, 2018 is 90.3%.
Key words, tags: tooth extraction, wisdom tooth, bone tissue, implant installation, augmentation, implantation.
Despite the rapid development of modern dentistry, tooth extraction is still a very common operation. When a doctor removes a tooth, be it a dystopic wisdom tooth or a severely rotted molar, in its place there remains a hole, a cavity, which is called the alveolar socket. Previously, the affected tooth was simply removed, and the resulting cavity, the socket, healed on its own, with a significant decrease in bone tissue. But today, when talking about qualified dental care, we should talk about preserving the alveoli in its original state, even in the absence of a tooth.
Anatomy of the alveolar process
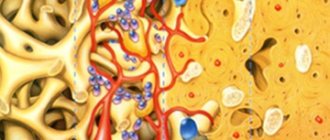
The alveolar, or dental, process (from Latin - processus alveolaris) is the part of the upper and lower jaws that extends from their bodies and contains teeth. The development and normal functioning of this structure is ensured by the roots of the teeth located in it. The alveolar process appears only after teeth erupt and almost completely disappears with their loss. After a tooth is removed, the corresponding area undergoes resorption (resorption). Dental alveoli, or sockets, are individual cells of the alveolar process in which teeth are located. They are separated from each other by bony interdental (interalveolar) partitions. Inside the alveoli of multi-rooted teeth there are also internal (intra-alveolar) interradicular septa, which extend from the bottom of the alveoli and divide the alveoli into chambers (according to the number of roots). The alveolar socket of the tooth has clear, defined boundaries, and it has all the conditions for bone regeneration; you just need to help it maintain its contour.
Tooth tissue
- Enamel: The most durable tissue in the human body, covering the surface of the dental crown. In terms of hardness, enamel is equivalent to crystal, since 97% of this tissue is inorganic.
- Dentin: the main hard tissue of the tooth. It consists of 70% hydroxyapatite, as well as water and organic material, fibers consisting of collagen, and dentinal tubules.
- Cement: tissue that covers the surfaces of the root and neck of the tooth. It is similar in hardness to bone. Cementum connects the alveolar bone to the tooth via the periodontal ligament.
- Dental pulp: loose tissue consisting of connective tissue fibers located in the tooth cavity. Rich in nerves and vessels (lymphatic and circulatory). Supplies dentin with nutrients.
Considering how a tooth is structured, one cannot exclude nearby tissues that support and strengthen the tooth.
- Periodontal ligament: fibrous tissue connecting the tooth root and alveolar bone.
- Alveolar bone: The jawbone that supports the tooth - it contains the sockets where each tooth is seated.
- Gums: soft tissue covering the alveolar bone.
- Gingival sulcus: a small space between the tooth and gum, the depth of which is between 1 and 2 mm. If this space deepens due to inflammation, a gum pocket is formed.
Based on their chewing function, teeth are classified into 4 types:
- The front teeth are incisors, used for cutting and grasping food.
- Fangs are cone-shaped teeth located next to the incisors, involved in holding and tearing food.
- The back teeth are small molars (premolars) and large molars (molars) that grind food.
Knowing the structural features of teeth, it is easier to find a common language with a dentist. You will feel confident and better understand the essence of the manipulations being performed.
Structure of the human tooth:
Hole preservation procedure
Preservation of the socket of an extracted tooth is a fairly simple and effective operation for preserving bone volume and maximizing the preservation of the natural contours of the alveolar socket. This surgical procedure is performed under local anesthesia and does not pose any risk.
Usually the operation is carried out in several stages:
- treatment of the hole after tooth extraction with special antiseptic compounds;
- installation of a membrane to protect the vestibular wall;
- filling the socket cavity with granular bone-forming substance;
- fixation of the operating surface by tensioning the free edges of the connective tissue;
- applying a bandage or a thin, neat suture.
Complete healing of the postoperative area occurs by the fourth week, and after 3–4 months, in some cases 6 months, if the condition is satisfactory, this area can be used to install an implant.
Pain in the tooth socket after extraction
If the tooth extraction operation is adequately carried out and all the dentist’s recommendations are followed, then after a couple of days the tooth socket should heal painlessly. A plaque forms at the site of damage, which is gradually covered by epithelial tissue as new bone tissue begins to grow.
And if pain persists after these days, it means that due to a combination of circumstances, inflammation has begun in the injured area (alveolus). In medical terminology, this process is called post-extraction alveolitis or alveolitis of the socket.
Etiology of alveolitis
After the tooth is removed, the created cavity should be filled with blood, which after a short time will transform into a special blood clot. Such a clot forms a biological barrier against all kinds of mechanical damage and infection.
But in some cases, the integrity of the blood clot is disrupted or for some reason it is completely absent, then the healing process is disrupted. In this regard, the development of alveolitis of the socket begins, which appears already on the third day and is accompanied by pain.
The main reasons for its occurrence and development are considered to be:
- Incorrectly performed surgery with violations of antiseptic rules, involuntary involvement of dental plaque in the socket, etc.
- Insufficient treatment of the postoperative socket, as a result of which small particles of tooth or pathological tissue remain in it.
- Complexity of the operation.
- Insufficient or complete absence of outpatient procedures for oral care recommended by a doctor.
- Failure to comply with simple hygiene standards.
- Eating food (especially spicy, hot or rough) before the recommended time.
- Self-medication by rinsing on the day of removal.
- Smoking in the first hours after tooth loss.
- Weak immune defense of the body.
- A number of common diseases that can affect the development of the inflammatory process.
Post-extraction alveolitis is dangerous due to severe consequences and complications. Therefore, this procedure must be approached responsibly and trusted to experienced and adequate specialists.
Symptoms and their manifestation
Usually, with a “dry” socket (no blood clot), the inflammatory process begins quite quickly after removal. Residues of food and saliva may be observed in an unprotected formation. Redness of the nearby gums is noticed, touching which causes pain.
If you do not seek medical help in time, the symptoms become more noticeable and are accompanied by:
- not soothing, rather severe pain in the damaged area;
- general condition worsens with rising temperature;
- a feeling of pain spreading throughout the entire jaw;
- the appearance of pus in the wound, resulting in a purulent odor from the mouth;
- formation of black plaque on the gum and socket;
- The submandibular lymph nodes gradually enlarge.
Emergency treatment at home
If the first signs of alveolitis appear and you cannot see a doctor within two to three days, you can try to alleviate the symptoms of the disease yourself.
It is important to remember that not all methods, drugs or folk remedies can cause relief. Some may even make the condition worse. For example, such well-known antiseptics as hydrogen peroxide or soda, on the contrary, will clean the infected hole beyond recognition, freeing it from blood clots, so that it will remain completely defenseless for infections.
If you can contact a specialist, you can use some types of analgesics to relieve pain. These include Baralgin, Ketanov or something similar. To relieve inflammation, you can rinse with a weak solution of potassium permanganate or furatsilin.
But natural antiseptics can be the most effective at home. Consider some folk recipes that have worked well for this disease.
Remedy No. 1
The herbal mixture has a good effect. Flax seed, blessed knycus, creeping tenacious (grass), blue cornflower (flowers), oregano, sunflower petals, are crushed and mixed in equal proportions. Then a spoon (tablespoon) of the crushed collection is filled with one glass of boiling water. The hour is running out. The strained mixture is divided into 4 doses and drunk throughout the day. Good reviews when using this decoction in the form of inhalation.
Remedy No. 2
Pour two tablespoons of St. John's wort (herb) and a spoonful of chamomile (flowers) into half a liter of boiling water and leave covered for two hours. Strain the resulting mixture and rinse your mouth with it at least every hour.
Remedy No. 3
A spoonful of medicinal sage is poured into a glass of boiling water. Brew for an hour in a thermos or wrapped in a thick thick cloth. After straining, rinse your mouth as often as possible throughout the day.
Remedy No. 4
A spoonful of dried chamomile flowers is poured into a glass of boiling water and steamed in a thermos for half an hour. Carefully filter and use as a rinse throughout the day.
Remedy No. 5
A decoction made from calendula (flowers) has an effective effect. A spoonful of flowers is poured with 200 ml of boiling water and steamed for half an hour. Then strain and rinse all day.
Of course, traditional methods of treatment can be effective, but it is better not to do without consulting specialists.
Treatment quality criteria
The main criterion for the quality of an alveolar socket preservation operation is its independent complete healing and maximum preservation of bone tissue, preservation of the natural contour and volume of the alveolar ridge, improvement of the condition of soft tissues and simplification of further stages of treatment. If the operation is successful, there will be enough bone tissue in the socket to install a dental implant. Separately, it is worth highlighting the advantages of condomization for the doctor and the patient - this is improved long-term treatment results, more predictable aesthetics and, of course, saving time for the doctor and the patient.
Indications for condom
Preservation of the socket of an extracted tooth is indicated for everyone who in the future wants to install a dental implant in its place. The process of loss and resorption of the jaw bone at the site of the extracted tooth begins immediately after the operation. In the first year, bone tissue resorption will be 25% in volume, and over the next 3 years the loss in width will be 40 - 60%. In the case of socket preservation after tooth extraction, a larger volume of bone tissue in the jaw and the most natural contours of the alveolar process are preserved. And then, subsequently, the likelihood of such a complex operation as alveolar bone augmentation when installing an implant will most likely not be required.
Something sharp sticks out of gum after tooth extraction
“I had a tooth removed, and now there is a sharp piece of root sticking out of my gum. What should I do?"
This is a fairly common complaint from patients after tooth extraction. Most patients are sure that a piece of a poorly removed tooth root is sticking out of the gum. In fact, this also happens sometimes, of course, but extremely rarely. But almost always the matter is completely different.
The tooth is located in the bone in its own socket, which follows the shape of its roots. The tooth socket smoothly transitions into the tooth, thinning along the edge. When a tooth is removed, the socket rises on its own, without the tooth inside. Naturally, the edge of the socket becomes the highest point of the bone in a given place, and since it is very thin, it becomes sharp to the touch. This sharp edge is called exostosis.
The first time after removal, the patient does not really notice such things, because... first anesthesia, and then swelling hide this sharp edge. And then the swelling goes away, and the bone begins to stick out through the thin mucosa. And this is already becoming noticeable both on the tongue and on the finger, with which patients, despite the ban, still regularly touch the extraction site.
Plus, the chewing process on such a sharp bone becomes very painful. The patient immediately blames the doctor for everything and does not even want to go to him, hoping that the “tooth fragment” will soon come out on its own. But, you understand, this is not a fragment and it will never come out on its own.
Therefore, there are only two ways to solve the problem.
The first and most correct
Contact the doctor who removed the tooth. The doctor will administer a small anesthesia and, under this anesthesia, gently smooth down the sharp edge. Sometimes with the help of a bur, and sometimes simply by squeezing the edges of the hole.
In any case, there is no need to remove the bone too much, because... it is very valuable for future implantation (if it is planned, of course). It is enough to simply smooth the edge of the bone slightly so that it does not scratch.
If implantation is not planned, then there is no need to remove a lot of bone either, because Even for a simple removable denture, bone is a very valuable resource. The more bone, the better the denture will fit on the jaw, the more stable it will be when chewing, the longer it will last, and the less bone will settle under the denture over the years.
The second method is a little dubious
If the protrusion of the bone is not so sharp, does not cause severe pain, and you cannot get to the dentist, then you can try to exercise the gum a little over this exostosis.
Old surgeons advised patients to smooth out such bone protrusions several times a day with an ordinary teaspoon or tablespoon. On the one hand, they still become smaller over time as a result of tissue resorption and sedimentation, on the other hand, such a massage causes thickening of the mucous membrane in a given place and the bone through such a “callus” is felt much less.
It is not so easy to smooth the bone by hand and cause the mucous membrane to grow, but they say that sometimes it works.
Contraindications
Preservation surgery is subject to the same restrictions as any osteoplastic surgery. Separately, I would like to note that it is not recommended to preserve a hole after tooth extraction in a state of acute pain, since the risk of complications increases. But in each specific clinical case, the actions of a professional dentist are strictly individual. Sometimes situations arise when you have to take risks, but this is due solely to medical indications. In any case, it is necessary to understand that performing a tooth extraction operation and subsequent preservation on a planned basis is better than as part of emergency care.
Restrictions
It is logical to perform a preservation operation after the removal of permanent molars, within the so-called sevens, second molars (except for wisdom teeth, eights), since when baby teeth fall out, bone tissue does not resorption. There is no upper age limit for performing an operation aimed at preserving the natural contours of the alveolar process.
Price
According to the classifier of surgical interventions in the oral cavity, condomation is not among the standard surgical interventions and this, of course, affects the cost of its implementation. In addition, the price of osteoplastic materials and related products is quite high. Some materials are used only in conjunction with a special membrane to avoid ingrowth of soft tissue into the alveolar socket. The price is also affected by the method of tooth extraction. Removal of a tooth or tooth root is sometimes still a traumatic procedure, leading to direct loss of alveolar bone and soft tissue. With atraumatic removal, the alveolar bone is preserved in a larger volume, which reduces the final cost of the operation.
Preservation of the socket after tooth extraction is an important procedure when planning the installation of an implant. Timely preservation of the socket will allow you to preserve such valuable bone tissue and avoid a much more complex and expensive operation to build it up - augmentation, as well as significantly reduce the overall treatment time. The cost of preserving the natural contours of the alveolar socket pays off, because you thereby provide the teeth surrounding it with a reliable position, and as a result, during implantation, you get an imitation of the removed tooth root. This procedure applies even to those patients who do not intend to restore or replace a lost tooth with an implant, because in this case the gingival contour will have the most aesthetic appearance, without failures, and will allow for the most aesthetic bridge prosthetics. Therefore, reservation is gaining increasing popularity in dental dentistry.
According to antiplagiat.ru, the uniqueness of the text as of October 16, 2018 is 90.3%.
Key words, tags: tooth extraction, wisdom tooth, bone tissue, implant installation, augmentation, implantation.
*Images: Astra Tech Dentsply Implants; Principles of hard tessue regeneration and implant therapy.
Tooth socket preservation technique
The literature describes many materials and methods aimed at preserving a fresh socket after tooth extraction, especially strengthening the relatively thin bone plate on the buccal side. Such methods include immediate implants after removal, bone replacement materials, as well as protective membranes, which in most cases allow only the level of the alveolar margin to be preserved. However, a method for completely preserving or regenerating the socket after removal has not been described.
The RST (root immersion technique) technique was described by Salama. Its purpose was to leave the root in the socket after removal of the coronal part, which led to complete preservation of the surrounding bone tissue, in contrast to other socket preservation techniques, which almost always result in resorption and, thus, a reduction in the height of the interdental papilla and the width of the alveolar margin. RST, on the contrary, imitates the natural apparatus of the tissues that support the tooth, which allows you to completely preserve the contours of the alveolar bone.
Also, in addition to leaving the whole root in the socket, there is a technique for preserving only its buccal part, after sectional cutting from the mesial to the distal side, forming two fragments: buccal and lingual/palatal.
This way, only the buccal fragment remains in the socket while the rest of the tooth is removed to make room for the implant.
This allows you to gain the bone preservation benefits of the RST technique while simultaneously placing an implant.
Clinical case
A 40-year-old healthy woman came to the clinic in order to replace the existing metal-ceramic prosthesis covering the upper central incisors, as well as to give a more aesthetic appearance to the front 4th incisors (Photos 1-4).
The two connected crowns “kept falling off,” the patient reported. Clinical and radiological examination revealed that the supporting stump of the right central incisor had collapsed, and only the root remained in the socket (photo 4), then the overgrown gum covered the root. There was no mobility or any periapical changes.
Photo 1: Front view
Photo 2: Right side view
Photo 3: Left side view
Photo 4
The connected crowns were essentially a cantilever prosthesis supported on the stump of the left central incisor (Figure 5).
Photo 5
The gingival growth is removed, the root is cut into two parts using a fissure bur in the mesiodistal direction, the lingual fragment is atraumatically removed (without pressure), then the buccal fragment is shortened using a surgical bur, leaving a thin layer on the side of the buccal bone plate (Photo 6-9) .
Photo 6: Sawed root
Photo 7: Lingual root fragment
Photo 8: Lingual root fragment
Figure 9: Intact buccal fragment
Approximately 1 mm from the remaining fragment, a direct implant KOS Single-piece (IHDE Systems) 12×3.2 was installed into the socket (Photo 10,11).
Photo 10
Photo 11
Two temporary crowns are installed on the left central incisor and the implant, all central and other functional contacts are removed. A post-intervention x-ray was taken (Photo 12).
Photo 12
A gentle diet is recommended during implant healing. The patient is advised not to load the area with the implant installed (Photo 13).
Photo 13
It took 5 months to heal. Afterwards, the existing stump and two lateral incisors were prepared (Photo 14).
Photo 14
Single zirconium crowns were installed on the 4 upper incisors (Photos 15-17).
Photo 15
Photo 16
Photo 17
Discussion
To overcome the negative consequences after tooth extraction, especially in people with a thin bone biotype, which is often prone to resorption in the apical and lingual directions, many techniques have been created using bone materials, protective membranes, etc. However, the technique of completely preserving the tooth socket and surrounding tissues to the present day moment was not described.
It is fair to assume that implants cannot perform the function of your own tooth in preserving the surrounding bone and soft tissue height.
Many studies to determine the safety of leaving roots in the alveolar bone have concluded that roots can be left in sockets, except in infected and mobile ones, as this can lead to rejection, infection and migration. In other cases, root fragments help preserve the structure of bone and soft tissue.
Flippi concluded that decoronation (removal of crown and pulp but preservation of root tissue) of an ankylosed tooth is a simple and safe procedure to preserve alveolar bone before implant placement.
Plata performed a 12-week histological examination of 12 retained roots, shortened to 2 mm below the bony margin. The data obtained indicated that 8 roots were completely ossified at the cut site.
An animal study was also conducted in which only the buccal portion of the root was preserved followed by implant placement. The root fragment did not interfere with ossification and helped preserve the thin buccal bone plate.
The major finding of histological analysis was that the internal space of the root was filling with new cementum and the formation of a new periodontal attachment.
On top of that, in places where the implant was installed in the root fragment, cement was detected on the implant itself. The same was determined in a study by Buser (1990), who concluded that in places where the implant was placed in close relationship with the root fragment, the implant itself was covered with a layer of cement with the inclusion of collagen fibers.
Nyman demonstrated that exclusion of epithelial cells leads to periodontal regeneration through periodontal ligament cells. It is also possible to assume that a blood clot between the root and the implant may prevent the proliferation of the epithelium. Amler and Cardaropoli demonstrated histologically that it takes approximately 4 weeks after tooth extraction for the socket to epithelialize. It can be assumed that similar processes occur between the implant and the remaining root fragment. If a blood clot prevents epithelial growth along the inner surface of the root, the remaining periodontal ligament cells regenerate to form a new periodontal attachment.
In contrast to these studies, Anthony Pogrel points out that late migration of the fragment is also possible in some cases, but it is considered impossible to determine this in advance.
In a pilot study conducted by Hermann, it was found that the amount of bone lost was much greater around a two-piece implant than around a single implant. Also, according to the state of the surrounding gums, the level of inflammation around the implant has an advantage on the side of one-piece structures.
Conclusion
It can be concluded that preservation of the buccal root fragment with simultaneous implantation is a reliable technique that promotes rapid ossification without any inflammatory process or resorptive effect.
But the study of long-term results and histological aspects of the technique remains desirable for further research of the technique.
Author: Haseeb H. Al-Dary, Private Practice, Amman – Jordan