Author: M. Cannon, N. Gerodias, A. Vieria, S. Persinoto, R. Yurado, Northwestern University School of Medicine, Department of Surgery, Children's Memorial Medical Center, Chicago, USA, San Paolo State University, Department of Pediatric Dentistry and endodontics, Aracataba, Brazil
Minimally invasive dentistry requires the use of conservative methods of restoring the dentition. But it is necessary to remember about the complications that may arise after this manipulation. The purpose of this nonhuman primate study was to compare the effectiveness of a novel light-curing pulp cap, TheraCal, Portland cement, synthetic calcium hydroxide, and glass ionomer in the treatment of bacterially infected pulp in primates.
Summary
The concept of minimally invasive dentistry is to use primarily conservative methods of dental restoration. This approach involves removing only those tooth tissues that cannot be restored, and relies more on the use of adhesive technologies rather than creating retention of the filling through a specific cavity design. However, even the use of the most modern adhesives does not exclude the possibility of marginal microleakage, which jeopardizes the vitality of the dental pulp.
In addition, even with gentle preparation, there is a risk of damage to the pulp. This may be facilitated by the anatomical and histological features of the teeth, such as a large pulp chamber, pronounced pulp horns or insufficiently formed, defective dentin. In such cases, maintaining the viability of the damaged pulp may require the use of a direct capping material that promotes pulp healing and the deposition of reparative dentin. Before suggesting the use of any of these materials in humans, the effectiveness of their use in animal studies should be assessed.
The purpose of this study was to compare the effectiveness of a new light-curing direct pulp capping material, pure Portland cement, polymer calcium hydroxide, and glass ionomer cement in the treatment of bacterially contaminated pulps in primates. Four individuals were included in the experiment, each of which had 12 teeth prepared under general anesthesia, exposing approximately 1.00 mm of pulp tissue on the buccal side. Cotton swabs soaked in a bacterial mixture consisting of microorganisms typically found in infected pulp were then applied to the exposed areas of the primate dental pulp. After removal of the packing, hemorrhage control and direct pulp capping were performed. The light-curing polymer material was applied using a needle and syringe to the exposed pulp areas of twelve teeth and then light-cured for 15 seconds. Pure Portland cement mixed with a 2% chlorhexidine solution was applied to the exposed pulp tissue of the other twelve teeth. An additional twelve teeth were treated with Triage Fuji VII glass ionomer cement (GC America), and the pulp of the remaining twelve teeth was capped with VLC DYCAL (Dentsply), a light-curing calcium hydroxide resin material. Fuji II resin-modified glass ionomer cement (GC America) was then applied to the base layer covering the exposed pulp. After 4 weeks, after the animals were killed, samples of the treated teeth were collected. These samples were demineralized, divided into fragments, stained and distributed into groups according to histological data. Statistical analysis of the obtained results was performed using the Kruskal-Wallis test.
When assessing inflammatory changes in the pulp, no statistically significant differences were found between groups (H = 0.679 with three degrees of freedom, P = 1.00). However, in both the Portland cement and light-curing pulp capping groups, hard tissue barrier formation was significantly more common by day 28 than in the GIC and Dycal groups (H=11.989 with three degrees of freedom, P=0.009). In addition, the thickness of the dentinal bridge in the first two groups was significantly greater than in the other two (H = 15.849 with three degrees of freedom, P = 0.002). The incidence of pulp necrosis in the GIC group was higher than in the other groups. Encouraging results achieved with a new light-curing material for direct pulp capping led to the development of TheraCal. Dentists quickly introduced TheraCal into their clinical practice as an easy-to-apply light-curing material for direct pulp capping. TheraCal does not interfere with standard techniques primarily used in clinical practice. Therefore, TheraCal can be successfully used as part of a dental restoration scheme using adhesive technologies, widely used in minimally invasive dentistry.
Direct coating of the pulp chamber with predictable results
There are a large number of clinical and research questions regarding pulp capping. For example, what is the best way to treat an asymptomatic tooth with moderate to severe caries, even though the removal of carious areas causes minor perforation of the pulp chamber? What materials are best to use? What can you learn about these procedures from already published sources? How much carious dentin must be removed to avoid perforation of the pulp chamber? Or should all tissues affected by caries be removed, regardless of the possibility of opening the pulp cavity? How to distinguish pathological dentin from damaged one? What materials should be used to control hemostasis in case of perforation of the pulp chamber? Questions regarding such a minor but extremely important procedure can be asked endlessly. The purpose of this article is not to answer all questions related to pulp chamber lining, but to briefly comment on the main points supported by research, literature and clinical experience.
Aggravating factors
Covering the pulp chamber is a surgical intervention that aims to preserve the vitality of the tooth and stimulate the formation of tertiary dentin in it. This topic has been researched for almost a century and continues to evolve as we now have a better understanding of pulp, dentin and their biological restorative capabilities. Despite new advances in research, this issue remains quite controversial, as leading experts, manufacturers, researchers, universities, associations and practitioners cannot agree on the best method to solve the problem.
Literature can help guide your work, but it can also lead you astray, since it contains both confirmation and refutation of most materials or techniques used by dentists. Rarely can the daily stressful work of a doctor be comparable to the everyday life of a researcher working in comfortable conditions. Considering all the above factors, many doctors, due to frustration or ignorance, resort to using old methods or materials instead of using the latest research, materials or techniques that may be a better alternative for their patients.
The prognosis for successful pulp cavity coverage (both direct and indirect) ranges from 13 to 100%. In the proposed sources, the prognosis for direct coverage of the pulp chamber is unpredictable with the lowest level of successful outcome of the procedure for perforation of the carious pulp cavity of adult teeth. A recent review of the literature by Cochrane in 2012 stated: “If existing extensive caries in a tooth is asymptomatic clinically, there is no clear consensus on the best treatment.” And it continues: “There is no consensus on whether direct or indirect pulp chamber capping should be used, whether the procedure should be done in two stages, or which material is most effective.” This statement appears to make it impossible for clinicians to obtain a confident answer as to whether the entire pulp needs to be removed or direct pulp coverage provided.
In clinical practice, when working with patients, they are guided by the proverb “hope for the best, expect the worst,” which sounds to patients like “root canal treatment is required and your tooth has a 50/50 chance.” Thus, the covering of the pulp chamber sometimes seems ambiguous. If a dentist uses this procedure as a conservative approach to save a tooth and it results in the development of irreversible pulpitis, the patient may be dissatisfied because his or her previously asymptomatic tooth now hurts and requires endodontic root canal treatment. On the other hand, if the tooth exhibits initial symptoms of pulpitis with little carious lesions and, in the opinion of the doctor, endodontic treatment is indicated, then the patient will end up with additional costs, effort, appointments and frustration.
Unfortunately, many insurance companies will not reimburse the cost of pulp chamber coverage if it is performed in one appointment along with the final restoration. In addition, some insurers simply do not allow the patient to be charged separately because reimbursement for a complete restoration includes pulp capping and the use of insulating and lining materials. This practice has led to a loss of motivation among dentists to provide services that will not be reimbursed, which may not be in the best interests of the patient. The costs associated with conservative pulp capping, as opposed to endodontic treatment, are less expensive, require less time to complete, and are more acceptable to the patient.
Diagnosis
There are many approaches to the procedure of direct capping of the pulp chamber, which consist of both direct capping whenever the pulp chamber is damaged, and the use of endodontic treatment when it is damaged. Some physicians in the association advocate the use of endodontic treatment for any perforated carious pulp cavity, regardless of its size or symptoms. However, clinical experience has shown that some carious lesions can be successfully treated with direct capping of the pulp chamber. The key to success is making the correct diagnosis.
It is often difficult to diagnose how inflamed the vital pulp is, or to what extent the infection has spread within it. The integrity of the pulp may be compromised and/or there may be a tendency to develop symptomatic or asymptomatic irreversible pulpitis, pulp necrosis, and/or symptomatic apical periodontitis (in which sometimes no changes are visible on radiographs). According to the endodontic diagnosis criteria adopted by the American Association of Endodontists (AAE), asymptomatic irreversible pulpitis is diagnosed on the basis of subjective and objective data, does not have any clinical symptoms, and the reaction to temperature stimulation is usually within normal limits; Moreover, such pulpitis most often occurs as a result of injury or deep caries. If these signs are detected, the doctor must make an informed decision regarding the need to perform direct/indirect pulp chamber covering or root canal treatment.
The AAE currently recommends root canal therapy in cases of asymptomatic irreversible pulpitis, but diagnosing pulpitis as irreversible without any clinical or radiological symptoms is challenging, so many clinicians opt for a pulp chamber capping procedure. It is worth noting that the American Academy of Pediatric Dentistry (AADP) clinical guidelines indicate that direct pulp chamber capping is applicable to permanent teeth that have minor carious or mechanical damage and when the pulp is in normal condition. This statement is contrary to the statements of other doctors and associations who recommend endodontic treatment for any carious lesion. However, it remains controversial that the pulp of a young tooth, with a better blood supply and higher regenerative capacity, provides a logical basis for guiding AADS.
Doctors are recommended to diagnose the condition of the pulp and apical tissues before necrectomy of carious tissues using comparative tests, such as biting, percussion, palpation, sensitivity to hot / cold / electrical stimuli, periodontal probing, determination of mobility, as well as x-ray examination for deep and advanced forms of caries. A thorough history and dental history should be documented along with a description of the chief complaint, history of the current problem (including onset, frequency, duration, intensity, location, precipitating factors, spontaneity, and mitigating factors), and clinical examination findings.
Removal of carious tissues
Understanding when to stop necrectomy of carious dentin can be complex and largely depends on the individual practitioner and his or her professional experience. Today, most doctors still rely on tactile sensation or dentin hardness. As you approach the pulp, it is recommended to stop excavation and leave a layer of softened dentin, but at the same time, some experts recommend starting endodontic treatment. Both approaches need to continue to be explored through designed, randomized controlled clinical trials. However, in a recent systematic review and meta-analysis of the literature in 2013, Schwendicke et al concluded that incomplete removal of carious tissue has advantages over complete necrectomy, especially in close proximity to the pulp. They also state that "there is currently no evidence to suggest that underprepared teeth are more susceptible to complications."
There are two options for partial necrectomy of carious tissues. The first, most commonly used by physicians today, is a one-step approach that is completed in one patient visit but has a higher failure rate. Despite this, a recent clinical study has provided encouraging results that carious dentin can be left intact with a one-step technique. This first option, in which a layer of carious dentin is left and a protective dressing is applied to deliberately prevent perforation of the pulp chamber, is known as indirect pulp capping. The second option, more effective due to its ultra-conservative nature, consists of two stages or two techniques, which include the installation of a temporary filling during the first visit after partial removal of carious dentin. At a follow-up appointment several months later (often 90 days, according to Dr. Stephen Wei's research), complete removal of all decay is completed with a permanent filling.
The second option, also known as a pulp-preserving step necrectomy, has received positive reviews in the literature, but many dentists do not perform this procedure due to multiple patient appointments, increased associated costs, lack of knowledge about the treatment, and possible due to problems related to insurance compensation. In addition, many patients want same-day permanent fillings rather than temporary fillings that require a follow-up visit over a 4-week to 12-month period.
Pathological dentin is softened tissue (demineralized or destroyed collagen) that has been destroyed due to the carious process and continues to retain bacterial contamination. In contrast, damaged dentin may be demineralized or softer than healthy dentin, yet retain its collagen structure and show no bacterial infection. Such damaged dentin may exhibit the ability to remineralize and should always be left to avoid perforation of the pulp chamber.
The layer of damaged dentin can be as thin as 1 mm, making it difficult to distinguish one type of dentin from another. Some clinicians and researchers suggest using a caries indicator solution whose chemical structure has been shown to bind to the denatured collagen of pathological dentin. However, many false-positive results have been recorded in the literature, as a result of which this technique remains controversial. Other options include the use of plastic or ceramic burs, enzymatic caries-dissolving agents, air abrasion, or laser ablation. Each approach has a special technique with its own advantages and disadvantages, and the doctor must thoroughly study each of them before settling on any particular one. Regardless of which technique or material is used, the clinician must completely remove peripheral carious dentin and work with extreme care to avoid damaging the pulp chamber during necrectomy of pathological peripulpal dentin.
Direct pulp opening
There are 3 types of direct pulp exposure: carious, mechanical and traumatic (Photos 1-3). Treatment of the latter two usually has a better chance of success due to the absence of infection of the pulp. Violation of the integrity of the pulp cavity due to the carious process, provided that the perforation is small and the diagnosis is correct, as indicated above, can be successfully treated by applying a pulp spacer (Photo 4).
Photo 1: Carious damage to the pulp cavity, greenish-yellow in color, with the possible presence of pus. Endodontic treatment of root canals is indicated.
Photo 2: Extensive carious perforation of the pulp chamber. Endodontic treatment is indicated.
Photo 3: A small combined opening of the pulp cavity due to mechanical and carious effects. Direct coating was performed without any complications.
Photo 4: Minor carious damage to the pulp chamber due to mechanical impact, the direct coating of which was performed without any complications.
During treatment of carious pulp damage, excessive pulp bleeding may be a sign of inflammation as well as a reduced ability to regenerate and form tertiary dentin. For hemostasis of pulpal perforations, it is proposed to use sterile saline solution, 2% chlorhexidine, sodium hypochlorite, ferrous sulfate, hydrogen peroxide, aluminum chloride, local anesthetics in combination with adrenaline and many other drugs. A cotton swab moistened with a hemostatic solution is applied to the perforation site for several minutes until hemostasis is achieved. If after several attempts this cannot be achieved, endodontic root canal treatment should be considered.
Most physicians use sodium hypochlorite because of its antibacterial properties and widespread use in endodontic procedures. However, it should be noted that it may interfere with the bonding procedure due to the release of free oxygen radicals. It is interesting to note that a number of studies have been published demonstrating an increase in the adhesive strength of dentin after pre-application of sodium hypochlorite. However, almost all of the above hemostatic agents, with the exception of saline and 2% chlorhexidine, can interfere with the adhesion process. Further research is needed to better understand this problem. Unfortunately, most hemostatic medications to a certain extent have cytotoxic properties and reduce the regenerative ability of the pulp. Despite cytotoxicity and deterioration of bonding, sterile saline, sodium hypochlorite, and chlorhexidine remain the drugs of choice for controlling hemostasis.
Materials used
Understanding when to perform pulp capping can be much more important than choosing the actual material to be used. In addition, the literature on this subject emphasizes that the marginal fit of the restoration is a more important aspect compared to the material used to cover the pulp cavity. Does this mean that any material can be used? Not necessary.
Over the past 5-10 years, a large number of materials and preparations for direct and indirect pulp capping have been introduced. Unfortunately, most new products require careful laboratory, biological and clinical studies. The increasing cost of conducting the latter under ever more stringent ethical standards, along with intense competition for grants, has contributed to the lack of clinical evidence required for the use of many of these new products, even if they have excellent characteristics. Many physicians, associations, and groups are reluctant to acknowledge the fact that it can cost more than $1 million to conduct a 1- or 2-year clinical trial. Even if they are carried out, the pilot batch size may not be sufficiently effective or the test results may not provide clear evidence regarding the feasibility of using the new product.
The development of test research structures (INIS) could help address some of these issues. Such systems conduct clinical trials of competitive products in various types of clinical activities. Although this method cannot control for every component, its strength is the number of activities in which these products are applied in natural conditions, which naturally can give a better idea of how the product will perform.
In a recent report of a clinical trial conducted by INIS, Hilton and others in 2013 evaluated and compared the likelihood of a favorable outcome of direct pulp capping of permanent teeth with MTA (Mineral Trioxide Aggregate) and CaOH (calcium hydroxide) with a significantly higher the likelihood of treatment failure with the latter. The authors concluded that MTA was superior to CaOH for direct pulp capping techniques. The authors of previously published clinical materials agree with this study, which confirms that MTA was either comparable or superior to CaOH in its characteristics. Unfortunately, these results were published 15 years after the product was introduced.
Although MTA has recently been demonstrated to be effective in the literature as a pulp chamber lining material, it is still not the primary agent used by most dental institutions. This may be due to its higher cost, crystallization time of 2 hours 45 minutes, or application method. Improved versions of the drug eliminate some of these shortcomings.
Most dentists use CaOH-based materials with varying degrees of success. As clinicians report, in the process of removing the restorative material under which CaOH was located, they discovered that the latter had completely disappeared or partially resorbed and crumbled. Hilton provided information in 2009 that self-curing calcium hydroxide preparations are highly soluble and may disappear completely over time. In addition, he said, they do not have sufficient adhesive properties and have poor sealing properties. In addition, the toxic effect on tissue of most CaOH-based pastes is described in detail in the literature. However, the material is inexpensive, easy to use, has a high pH that causes the release of bioactive molecules, and has antibacterial properties.
Other materials for direct pulp capping, such as those containing polyacrylic acid (eg, resin-modified glass ionomer cement, glass ionomer, and polycarboxylate cement), have also been used and investigated with varying success. Despite their biocompatibility and considerable attention from some authorities, all of these materials are toxic to the pulp, and their polyacrylic acid inhibits the formation of apatite, which casts doubt on their value for direct pulp capping techniques. MTA or CaOH based materials used as a liner or base liner on damaged dentin or other material used in the direct pulp capping process have demonstrated their suitability and are therefore recommended for use. Many dentists believe that the high concentration of fluoride released initially by these products makes them ideal materials for direct pulp capping applications. However, as reported in the literature, the release of fluoride from these materials increases the toxic effect on pulp stem cells. Moreover, manufacturers of these types of materials do not recommend them for direct pulp coating, most likely precisely because of the high level of fluoride released, which is toxic to pulp cells.
Adhesives have been researched and used for some time as pulp capping materials. Their use would save time and expense, but unfortunately they are toxic to pulp cells, which reduces regeneration, leads to chronic inflammation and poor sealing. Choosing zinc oxide eugenol for pulp capping may seem like a logical choice since it has been successfully used in many other areas of dentistry, including temporary restorations. However, when used for direct pulp capping purposes, it can lead to inflammation, weak dentin bridges, microleakage, and decreased pulp regeneration.
Biological activity
Terms such as “bioactive,” “bioavailable,” and “bioactive” are now widely used by some manufacturers and authorities to make claims about their newest products and as phrases used to attract customers and increase sales. From a research point of view, the term "bioactivity" was first described more than 25 years ago during the study of glass-ceramic materials, since the formation of an apatite layer is a necessary and sufficient condition for bioactivity (Kukubo T. et al., 1990). Subsequently, the concept of “bioactivity” was defined according to the ISO 23317:2014 classification in surgical implantology as “the ability to cause a specific biological reaction on the surface of a material, which leads to interaction and adhesion between tissue and material.”
This document is applicable to implant surfaces that come into direct contact with bone tissue; its application to restorative materials is not necessary. In other words, bioactivity implies the formation of a layer of apatites and the formation of a bond between the tissue and the material, which most likely occurs due to the deposition of apatites. To date, several new bioactive materials have demonstrated this, but only in vitro. Further clinical research studies are required to actually confirm that these materials actually cause the formation of hydroxyapatite and bonds between dentin and the pulp capping material.
In a recent review article by Niu, Pashley, Tay, et al., published in 2014, the authors conclude that “generally accepted criteria are not sufficient to objectively assess bioactivity relevant to a living organism” and that “the term “bioactivity” used very ambiguously." They recommend that ISO (International Organization for Standardization) or ASTM (American Society for Testing and Materials) develop evaluation criteria and precisely define the term “biological activity” used in restorative and endodontic procedures. This would make it possible to better determine development vectors and more accurately outline the developing branches of restorative and endodontic dentistry.
Despite the above inaccuracies in determining whether a drug is bioactive or not, several new materials have emerged that are similar in action to MTA. The manufacturers of these materials managed to create a product without the disadvantages inherent in MTA. These materials are currently used in practice due to the successful results of clinical trials. TheraCal LC from BISCO and Biodentine from Septodont are two newer products that are similar to MTA in terms of their properties and being calcium silicate cements. Both materials contain calcium silicate fillers that release calcium and hydroxide ions, which stimulate the formation of apatite, promoting regeneration and healing due to the alkaline pH (and its antibacterial effect). The materials also contribute to the release of biologically active dentin matrix proteins and the formation of a layer of secondary dentin.
Both materials are being actively researched, but more clinical trials are needed to confirm the factors that many dentists consider to be critical in the direct pulp chamber capping technique. The differences between the two products are in the procedure for use, indications for use and methods of application. TheraCal LC is a light-curing material designed for direct and indirect pulp capping techniques, while Biodentine, which crystallizes in 12 minutes, can also be used for endodontic procedures by pre-mixing it in a triturator (amalgam mixer).
Calcimol LC (VOCO) and Activa (Pulpdent) are materials that the manufacturers claim have biological activity due to the release of various ions, including calcium ions (Activa also contains fluoride and phosphate ions). Calcimol LC is a polymer-based calcium dihydroxide and is similar to the other light-curing CaOH-based polymer pastes described above. Activa is a dual-cure base/liner that contains a bioactive polymer matrix and bioactive fillers. Regarding their ability to form bonds between tissues and materials or form apatite crystals, only a small number of studies have been performed. It should be noted that the above two materials are not indicated for use in direct pulp capping. In particular, Activa releases large amounts of fluoride, which can be toxic to pulp cells.
Pros and cons
According to research, good marginal adaptation is the key to successful and durable adhesive restoration, and can also stop further progression of carious lesions. Failure to do so results in tooth extraction, endodontic treatment (root canal treatment) or diagnosis of pulp necrosis, irreversible pulpitis, apical periodontitis or apical abscess. Successful diagnosis of a tooth using the method described above and ensuring a good marginal seal of the filling using rubber dam insulation can lead to:
1. Resorption of the tooth over a period of time, which can be months, and the potential for long-term sensitivity. Clinicians should periodically monitor for any radiographic changes that are symptoms of apical periodontitis.
2. Gradual deterioration of the tooth over a short period of time, requiring either emergency pulp extirpation and/or medicinal root canal treatment.
3. Gradual deterioration of the tooth over a long period of time, with the patient being able to endure the pain until one day he can no longer cope with it, eventually leading to an emergency pulpectomy or medicinal root canal treatment.
Factors influencing success or failure include: size of pulp chamber injury, amount of bleeding, type of injury (carious, mechanical, or traumatic), use of rubber dam, drug used to control pulp bleeding, absence of symptoms, type of restoration performed (temporary or permanent), and restoration class (I or II).
Clinical case
A 14-year-old female patient presented for routine dental restoration on a maxillary molar with no complaints or signs of pain sensitivity. X-ray and clinical examination revealed a moderate to severe carious lesion on the occlusal surface of the tooth. After anesthesia and isolation of the working field using a rubber dam, access to the tooth was created using a carbide bur. During the necrectomy (excavation of carious tissue), the mesial wall of the pulp chamber was perforated, causing moderate bleeding (Photo 5). Upon examination, it turned out that the cause of its damage was carious-mechanical impact. A cotton swab moistened with 2% chlorhexidine solution was placed in the perforation area until bleeding stopped. A new medicated cotton swab was used to disinfect the remaining walls of the prepared cavity.
Photo 5: Moderate combined mechanical perforation of a carious pulp cavity. Hemostasis has been achieved.
TheraCal LC from BISCO was used in small quantities to directly coat the pulp chamber (Figure 6). The material was applied by grabbing a few millimeters around the edges of the perforations to ensure a good seal, after which it was light-cured for 20 seconds. Following the total etching technique, adhesive was applied to the top of the pulp chamber and adjacent dentin (Figure 7). The traditional composite was layered, processed and polished (Photo 8). The procedure was completed with the patient warned of the possible need for root canal treatment if the pulp cavity did not recover.
Photo 6: Application of BISCO TheraCal LC to exposed pulp cavity and adjacent dentin.
Photo 7: Etching the enamel and remaining dentin with phosphoric acid.
Photo 8: Polymer composite material is applied in layers on top of the pulp protector.
Subsequent appointments revealed no signs of sensitivity or complications (Figure 9). Regular radiological and clinical examinations have been carried out over the past 3 years.
Photo 9: View of the restoration after 3 years.
conclusions
Prediction of the outcome of pulp chamber coating in everyday practice can be significantly improved by following strict rules for dental diagnosis before the start of necrectomy (excavation of carious tissue). Using extreme caution, try not to damage the pulp chamber by removing only pathological dentin and performing indirect coverage of the pulp cavity with proven materials that will promote its regeneration and stop the further spread of the carious process. During direct pulp capping, disinfect the cavity and control bleeding with 2% chlorhexidine, sterile saline, or sodium hypochlorite. Use MTA with a glass ionomer/glass ionomer polymer liner/base or newer MTA-like materials that offer many benefits over traditional CaOH-containing formulations. Finally, ensure that the restoration is well sealed under rubber dam conditions.
Authors: Paul L. Child Jr. , DMD, CDT Mark L. Cannon , DDS, MS
Introduction
An ideal material for direct pulp coating should have a bactericidal effect, should not have a negative effect on the pulp and other tissues of the oral cavity, and should activate regenerative processes in the pulp. Various substances have been proposed for these purposes, such as lyophilized bone, collagen, morphogenetic proteins and allogeneic dentin matrix, as well as non-pharmacological treatment methods, such as laser and electrosurgery. The properties of calcium hydroxide, such as biocompatibility, the ability to stimulate the formation of a mineralized barrier, a high acidity level and the associated bactericidal effect, also allow it to be considered as a material for direct coating of dental pulp.
Loma Linda University, California, has proposed a new drug called mineral trioxide aggregate (MTA) designed to close communications between the root canal system and the outer root surface at various levels. Mineral trioxide aggregate consists of small hydrophilic particles (powder) that harden in the presence of moisture. Its main components are: tricalcium aluminate, tricalcium silicate, calcium oxide and silicon oxide. All of these substances are constituents of Portland cement, with the exception of bismuth oxide, which was added to MTA to impart radiopaque properties. Using electron microanalysis, it was established that the main ions present in MTA are calcium cation (Ca2+) and phosphate anion (PO43–), and since they are also the main components of dental tissue, the latter are biologically compatible with this drug. Once mixed with water, the material's acidity level increases from pH 10.2 to pH 12.5 over the next three hours, giving it antimicrobial properties against certain facultative anaerobic bacteria. This drug is characterized by excellent sealing properties, biocompatibility, lack of mutagenic activity, low cytotoxicity, and the ability to stimulate a cellular response, resulting in the deposition of cement on the root surface, which promotes the regeneration of the periodontal ligament and the formation of bone tissue.
Holland and colleagues showed that MTA, which contains, among other things, calcium oxide, acts similarly to calcium hydroxide: when the powder is mixed with water, calcium oxide is converted to calcium hydroxide. Upon contact with tissue fluids, calcium hydroxide dissociates into Ca2+ and OH– ions. Calcium ions react with carbon dioxide in tissues, causing the deposition of limestone granules. In parallel with the deposition of the mineral component, fibronectin accumulates, which promotes cell adhesion and differentiation. Over time, a hard tissue barrier forms.
Pitt Ford and co-workers studied the response of pulp tissue after coating it with MTA and Dycal and found the presence of dentinal bridges after 6 months in the pulp of all teeth treated with MTA, while in the group where Dycal was used, all teeth showed signs of severe chronic inflammation and only two cases of dentin bridge formation. Abedi et al found that MTA resulted in less inflammatory response and greater calcification than Dycal for direct pulp capping in dogs and monkeys. Previous studies have demonstrated the formation of dentin bridges following direct pulp capping with VLC Dycal, a light-curing, polymer-based material containing calcium hydroxide. Pitt Ford and Roberts studied the response of the pulps of 64 teeth of four cynomolgus monkeys to mechanical exposure followed by direct coating (immediately or after 24 hours) of Dycal, VLC Dycal, or Prisma-Bond. Dentin bridge formation was found in almost all teeth treated with Dycal or VLC Dycal, and pulp inflammation was observed in only one tooth, indicating infection. However, the success rate in the delayed pulp capping group was as high as in the immediate capping group.
Holland showed that pulp capping with both MTA and Portland cement promoted the formation of dentinal bridges after pulpotomy in dogs. Estrela reports that MTA and Portland cement have comparable antibacterial activity. Saidon and Menezes also showed that the use of MTA and Portland cement as direct pulp capping materials produced similar histological results. It was therefore no surprise that Funteas found no significant differences when comparing 14 different elements of Portland cement and MTA. De Deus and co-workers compared the cytotoxicity of ProRoot MTA and MTA Angelus with Portland cement and found no statistically significant differences between the materials.
Additional methods of conservative treatment of pulpitis
Physiotherapeutic treatment is used as an addition to the biological treatment method. The following procedures are shown:
- Helium-neon laser - its radiation has an analgesic effect, helps reduce swelling, reduce inflammation.
- Electrophoresis - using this method of electrotherapy, anesthetics are injected into the site of inflammation.
- Ultrasound therapy – low-frequency ultrasound stimulates regenerative processes and accelerates the delivery of medicinal substances to tissues.
After treatment of pulpitis with a biological method, patients must undergo electroodontic diagnostics in order to monitor the condition of the pulp. If the electrical excitability of the pulp is not restored after treatment and pulp death is diagnosed, a depulpation procedure (pulp removal) is performed.
Materials and methods (study on primates)
The experiment included four individuals, young male Capucin Cebus Opella, which were randomly selected from the primate population of the Monkey Research Center, Aracataba, Sao Paolo. The study design was approved by the Animal Research Committee of the University of São Paulo, Aracatuba, Brazil. Throughout the experiment, animals were cared for in accordance with international standards. All procedures were performed in the primate operating room of the Monkey Research Center. According to the established research plan, 12 teeth were prepared from each primate with penetration into the pulp tissue from the buccal side. The dissection was carried out under general anesthesia with thiopental 30 mg/kg intramuscularly and diazepam 17 cm3 intramuscularly under sterile conditions. The teeth were previously cleaned of plaque and isolated using a rubber dam. Disinfection of the surgical field was carried out with providone iodide. Tooth preparation was carried out using small high-speed handpieces (Dabi Allante). Before each use, the tips were autoclaved. A new sterile small spherical bur was used for preparation. The surgical field was cooled with a sterile isotonic solution. The cavity was formed within the enamel, expanding it in the mesiodistal direction. The preparation was completed by opening the pulp chamber in the center of the formed cavity in an area with a diameter of 1.0 mm (Fig. 1). After completion of the preparation, the exposed pulp tissue was irrigated with a sterile isotonic solution to remove dentinal filings.
| Rice. 1. Isolation, disinfection and preparation of primate teeth. An area of exposed pulp measuring approximately 1.0 mm is located in the center of the prepared cavity |
Cotton swabs soaked in a bacterial mixture consisting of anaerobic and aerobic microorganisms typically present in infected pulp were placed on exposed areas of primate dental pulp. This mixture contained Porphyromonas gingivalis and Fusobacterium nucleatum, since both of these species are known to cause acute pulpitis and apical abscesses. After bacterial inoculation (with an exposure duration of 30 min), the pulp tissues were immediately washed with a sterile isotonic solution. Cotton swabs soaked in Cipro HC Otic solution were then applied to the infected pulp for 5 minutes. After removal of the swabs containing the solution, bleeding control and direct pulp capping were performed.
Light-curing polymer cement for direct pulp capping was applied to the pulp of 12 teeth at the tip of a syringe needle and light-cured for 15 s. Pure Portland cement mixed with a 2% chlorhexidine solution was applied to the exposed pulp of the other 12 teeth. An additional 12 teeth were treated with GIC (Triage, Fuji VII, GC America), and the pulp of the remaining 12 teeth was coated with VLC DYCAL (Dentsply), a light-curing resin material containing calcium hydroxide. Polymer-modified GIC (Fuji II LC, GC America) was then applied to the base layer of direct pulp capping material.
All monkeys were cared for during the experiment in accordance with international animal care standards. The primates were monitored for any changes in eating habits or signs of inflammation or suppuration of the oral tissues. At the discretion of the animal care staff, analgesics were administered when necessary. The behavior of the primates was carefully observed, and all data was recorded. No changes in behavior were observed in any of the animals.
4 weeks after the animals were killed, samples of the prepared teeth were collected and serial sections of tissue 6 mm thick were carried out using a Leica BM 2025 microtome. The preparations were stained using the following methods: hematoxylin and eosin staining, brown and brown staining, Masson trichrome staining . All specimens were submitted to Northwestern University for independent histological evaluation. Histological examination of the specimens was carried out using a Leitz Dialux 20 microscope. The personnel conducting the independent assessment were not aware of what materials and techniques were used, since all specimens were identified only by location. Histological analysis was carried out according to the following parameters: • the presence of necrosis, hyperemia, • the thickness and quality of the hard tissue barrier, • the presence of odontoblasts, the presence of other foci of calcification, • the presence of gigantocytes, • the presence of particles of pulp covering material (Table 1). The severity of inflammatory changes was assessed on the following scale: • no signs of inflammation – 0, • mild inflammation – 1, • moderate inflammation – 2, • severe inflammation – 3, • abscess formation – 4.
Table 1. Results of histological examination
| Inflammation scale | TheraCal | Portland cement | GIC | Dycal |
| 0 | 7 | 4 | 3 | 2 |
| 1 | 1 | 4 | 1 | 2 |
| 2 | 1 | 2 | 3 | 4 |
| 3 | 1 | 1 | 1 | 3 |
| 4 | 1 | 1 | 3 | 0 |
Dentin bridge thickness was measured (Fig. 2) using a phase contrast microscope using three randomly selected points on two different sections of each specimen. Statistical processing of the data was carried out by independent specialists.
| Rice. 2. Example of a histological specimen after application of a light-curing pulp capping material showing measurement of the dentinal bridge. Odontoblast-like cells accompanying the bridge are also visible, and there are no signs of inflammation |
Treatment of deep caries of permanent teeth
Jerod Johnson, DDS
Vital treatment methods are widely used in modern dentistry. We typically prevent or remove carious lesions using a variety of treatment options. However, the question of endodontic treatment of permanent teeth with deep carious lesions in children remains open.1,2
There are several methods for treating deep caries of permanent teeth in children and adolescents. Their main goal is to preserve the vitality of the pulp without leading the process to endodontic treatment or removal of a permanent tooth. In cases where pulp necrosis is already observed, especially in teeth with immature roots, treatment becomes difficult due to:
- thin dentinal walls prone to cracking
- a large number of pulp decay products
- difficulty in canal irrigation
- lack of apical stop
Preserving pulp vitality is the key to achieving apexogenesis, which in turn leads to physiological formation of the root apex.3–5 In addition to difficulties in diagnosing diseases and dental anatomy, the child's behavior in the dental chair can also cause discomfort.6
Developments in the use of calcium silicate formed the basis of ProRoot MTA, which has proven effective in treating deep caries in permanent teeth with immature roots.7 Mineral trioxide aggregate, or MTA, is a biocompatible material consisting of tricalcium and dicalcium silicate. The material has been successfully used for both indirect and direct pulp capping, and for partial and complete pulpotomies in permanent teeth.8
When MTA binds to the intercellular fluid, it releases calcium, which in turn is part of hydroxyapatites.9 This manifests itself in a chemical bond with dentin and sealing of the dentinal tubules.10 The alkaline environment of MTA creates unfavorable conditions for bacteria and ensures sufficient tightness in the canal.11 -12
The hardening time of MTA ranges from two to four hours, and therefore it is impossible to immediately perform permanent obturation of the root canals. Disadvantages also include the high cost of the material and difficulty in handling it.7
Thus, when MTA comes into contact with sodium hypochlorite, the tooth may turn dark. Staining may also be associated with bismuth oxide, which is part of radiopaque filling pastes. Other chemicals lead to less pronounced dental discoloration.13
results
Statistical analysis of the results was performed using the Kruskal-Wallis test. There were no statistically significant differences between groups regarding the severity of pulp inflammation (H=0.679 with three degrees of freedom, P=1.00). However, in both the Portland cement group and the light-curing pulp capping group, cases of dentin bridge formation by day 28 (Table 2) were significantly more common than in the GIC and VLC Dycal groups (H= 11.989 with three degrees of freedom, P=0.009). Dentin bridge thicknesses in the Portland cement and light-cured pulp capping groups were also statistically greater than those in the other two groups (H=15.849 with three degrees of freedom, P=0.002). In addition, the number of cases of pulp necrosis in the GIC group was higher than in the other groups.
Table 2. Formation of a hard tissue barrier by day 28
| Presence of a barrier | TheraCal | Portland cement | GIC | Dycal |
| Yes | 11 | 12 | 4 | 4 |
| No | 1 | 0 | 8 | 8 |
Direct pulp capping
Initially, direct pulp capping was performed using calcium hydroxide.17 The action of calcium hydroxide is based on the induction of coagulative necrosis in the superficial layers of the pulp and on the stimulation of dentin bridge formation. Subsequently, the calcium hydroxide dissolved, causing pores to form in the replacement dentin; in 89%, defects in the formed dentinal tubules were observed after 2 years.18 Given the possible risks of breaking the seal of the restoration, this material was soon abandoned.
Also, the formation of the dentinal bridge took much longer with calcium hydroxide compared to MTA.19 A recent study on direct pulp capping showed a significant advantage of MTA over calcium hydroxide. It is important that, regardless of the use of one or another material, replacement dentin was formed in the area of the pulp horns.20
Clinical case 3: Treatment instead of removal
An 8-year-old patient complained of the first lower permanent molar on the left. After the examination, it was recommended to remove the permanent molars due to the presence of deep carious cavities and deformation of the dentition due to the early removal of temporary molars. The family refused removal and decided to treat the tooth. Reversible pulpitis was diagnosed in tooth 3.6. The tooth was anesthetized and the tooth was isolated with a rubber dam. The tooth cavity was prepared and the pulp was exposed. The tooth was medicated with sodium hypochlorite solution, after which ProRoot MTA was applied in the area of pulp opening using an amalgam tray and a cotton ball. A damp cotton ball was placed on top of the material, temporarily sealing the cavity with IRM cement. The tooth was later restored with composite material. 2 years after treatment, the patient was not bothered by the tooth, and the radiograph did not reveal any periapical changes.
Clinical methods
The patient came for planned treatment for recurrent caries at the border with an incompetent restoration occupying the chewing and lingual surfaces of the tooth. Before this appointment, he had no complaints of increased sensitivity or discomfort. After local anesthesia, a rubber dam was applied. After removal of the old restoration, microleakage of the filling and, as a consequence, resorption of the lining material was discovered. Further removal of the infected tooth tissue led to the opening of the pulp (Fig. 3). When the lingual fissure was stained with a caries detector, there were no signs of demineralization, so there was no need for its excision.
| Rice. 3. Pulp exposure in an asymptomatic molar. During the careful removal of carious dentin, one of the pulp horns was opened. Careful hemostasis must be performed before continuing treatment. |
Bleeding from the pulp tissue was stopped by applying a sterile cotton swab soaked in a solution of local anesthetic (Fig. 4). Other recommended solutions to stop bleeding are ferrous sulfate, sodium hypochlorite, 2% chlorhexidine (Cavity Cleanser, Bisco). Regardless of which solution is used, the clinician should be careful to ensure that it does not interfere with the adhesion of permanent restorative materials.
| Rice. 4. After the bleeding has stopped, it is clearly visible that the exposed area of the pulp is much smaller than it seemed at first |
When applying the new polymeric light-curing material (Table 3) to cover the TheraCal pulp, apply pressure to the syringe plunger for only 1-2 seconds. When the material begins to flow out of the syringe, apply a small ball of material that forms at the end of the needle to the bottom of the prepared cavity. The material is easily distributed with a needle and completely covers the exposed pulp area as well as approximately 1 mm of surrounding dentin. The applied layer should be less than 1 mm thick, ideally 0.3-0.5 mm. In Fig. Figure 5 shows that the pinkish pulp tissue is still visible through the layer of covering material. After application, TheraCal is polymerized for 20 seconds with a light flux density of at least 500 mW/cm2.
| Rice. 5. Application of light-curing pulp capping material |
After the material has polymerized, the doctor can begin traditional bonding and restoration procedures. In this case, the tooth was restored using a “total etching” technique and using a low-shrinkage composite material (Fig. 6). The prepared cavity was treated with 32% Semigel etchant with benzalkonium chloride (Bisco Inc, USA) for 30 s. The etching gel was applied first to the enamel and then to the dentin for 10 s. After rinsing the cavity, excess moisture was removed, leaving the dentin moist.
| Rice. 6. “Total etching” technique with 32% BAC gel applied first to the enamel and then spread onto the dentin. The cavity is washed abundantly with water. Excess moisture is carefully removed using a powerful vacuum cleaner, leaving the dentin moisturized. Two layers of One Step adhesive are then applied and light cured before filling the cavity with a modified GIC and low shrinkage composite material. |
Then two layers of One Step adhesive (Bisco Inc, USA) were applied and cured with light. The cavity was filled using the sandwich technique. The first layer of polymer-modified GIC was applied up to the enamel-dentin border. The tooth was then restored with packable composite material Aelite LS, which was applied first to the edges of the cavity and then reproduced the anatomical shape of the tooth (Fig. 7). Each layer of material was cured for 20 s with a light output of at least 500 mW, first on the buccal side, then on the lingual side, and finally on the surface. The last layer was smoothed using a Thomas float, then a layer of BisCover surface sealant was applied. After light curing of the sealant layer, the rubber dam was removed and the occlusion was checked. The surface can then be polished in the usual manner using carbide finishes and rubber heads.
| Rice. 7. Apply the last layer of Aesthetic LS, color A1, and form the anatomical structure of the tooth using a plugger. To improve the surface characteristics of the restoration, BisCover sealant was applied |
Follow-up is necessary in all cases where pulp viability may be compromised. The patient was warned to call immediately if any symptoms occurred, with particular attention to temperature sensitivity or discomfort when biting on the tooth. If these symptoms appear, an X-ray examination is indicated, and then, if necessary, endodontic treatment. The patient did not complain of any symptoms during the follow-up visit (Fig. 8).
| Rice. 8. Repeat visit 6 months after treatment. The patient does not complain of increased sensitivity after rehabilitation therapy |
Partial pulpotomy according to Cvek
Cvek pulpotomy is named after Dr. Miomir Cvek, who promoted the partial pulpotomy technique. This method involves removing necrotic pulp or part of the exposed pulp, leaving only healthy pulp in the apical zone in order to maximize the preservation of viable tissue in the dental pulp. Next, healing material is placed to cover the remaining pulp.21
For many years, calcium hydroxide was used for pulp capping, but soon calcium silicate, such as the mineral trioxide aggregate, began to show mixed results in treatment.22 The preservation of viable pulp was demonstrated in a histological study in which a response remained with caries progression. sides of the pulp. As caries progressed, the pulp began to react to bacterial invasion; research has shown that even in the presence of inflammation, necrosis in the coronal portion of the pulp, there may still be healthy pulp underneath.23
Clinical case 4: Accidental opening and subsequent restoration of a tooth
An 11-year-old boy complained of pain in the lower jaw on the left. Previously, he had consulted a dentist, who prescribed him a course of antibiotics and referred him to an endodontist for root canal treatment, but the patient was never able to visit a specialist. The patient reported mild, intermittent tooth pain.
When examining tooth 3.6, a deep carious cavity was revealed on the chewing surface. The cold test was positive, the pain disappeared immediately after the removal of the irritant. The x-ray revealed a deep carious cavity with damage to hard tissues of more than 2/3, the stage of an unformed root. Diagnosis: reversible pulpitis without pathological periapical changes.
Anesthesia was performed and the tooth was isolated using a rubber dam. Next, the carious cavity was prepared and the tooth pulp was exposed. After which a partial pulpotomy was performed with a diamond bur from Komet USA, and the remaining pulp was treated with 6% sodium hypochlorite (Vista Dental). ProRoot MTA (Dentsply) was applied to the exposed tooth cavity using an amalgam tray and a cotton ball. The tooth cavity was closed with Fuji IX glass ionomer cement (GC America), and then the tooth was restored with Filtek Supreme composite material in color A2B (3M).
At the re-appointment, the patient had no complaints, and the radiograph did not reveal any periapical changes. Preventive examinations are necessary to monitor the process of apexogenesis.
Discussion
Portland cement (MTA) fully satisfies the requirements for it in cases of treating teeth with exposed pulp. • Although both glass ionomer cement and light-curing polymers containing calcium hydroxide are also recommended for direct pulp capping, they are not the materials of choice. • On the other hand, MTA or pure Portland cement is difficult to apply and takes too long to set. • TheraCal is easy to apply and cures within 20 seconds of curing. TheraCal powder continues to harden due to the penetration of water into the hydrophilic polymer matrix, which increases the strength properties of the material. In addition, the alkaline pH and the presence of calcium oxide in its composition determine the biocompatibility and antibacterial properties of this material.
Table 3. Acidity level of different versions of TheraCal and Dycal VLC
| Day | TheraCal A | TheraCal B | TheraCal C | Dycal |
| 1st | 11,191 | 10,911 | 11,288 | 8,599 |
| 28th | 9,327 | 8,606 | 9,667 | 7,868 |
| 168th | 8,738 | 7,894 | 8,752 | 7,619 |
| 265th | 8,481 | on day 175 pH = 7 | 8,466 | on day 170 pH < 7 |
Light-curing TheraCal has found rapid clinical acceptance as a material with good adhesion to wet substrates. A small amount of material can be syringed into the deepest part of the cavity or applied to the exposed pulp. TheraCal, after polymerization, is firmly retained in the cavity and is not washed away during the etching and rinsing procedure. In addition, a very thin layer of material is sufficient to create the desired effect. Of course, the TheraCal layer should not be too thick, since in this case it will not completely polymerize. In addition, a thick layer can compromise the strength characteristics of the permanent restoration. In appearance, TheraCal material is similar to tooth enamel, so its use does not cause problems from an aesthetic point of view.
To date, none of the patients we have treated with TheraCal have complained of hypersensitivity or experienced complications. Of course, this information, based on anecdotal evidence, as well as our extensive clinical studies, needs to be confirmed by the long-term positive results of using this light-curing direct pulp capping material.
Pulpotomy
Pulpotomy is a fairly common technique in the treatment of temporary teeth, and the use of this technique in the treatment of permanent teeth is also increasing. A systematic review reported a success rate of 89.6% when performing pulpotomy in primary teeth using MTA.24 The properties of MTA are applicable to pulpotomy in permanent teeth. More recently, the material has also been shown to be successful in teeth with symptoms of irreversible pulpitis.25
Clinical case 5: Irreversible pulpitis
The patient was diagnosed with irreversible pulpitis in tooth 4.6. The X-ray showed an immature apical stage. After anesthesia and the application of a rubber dam, the carious cavity was prepared. Viable pulp tissue was visible in the opened tooth cavity, and hemostasis was performed. Hypochlorite solution was used as a medicinal treatment, and ProRoot MTA was applied to the opened tooth cavity.
A damp cotton ball was placed over the MTA and the tooth was sealed with temporary IRM cement. The tooth was later restored with a metal crown. During subsequent visits, the tooth remained asymptomatic and further root formation was observed.
Acknowledgments
The authors would like to express their appreciation for the invaluable assistance provided by Drs Arthur Weiss and Dr Stuart Stock, without whom this project would not have been possible. We would also like to thank Dr. Eugene Lautenschlager for the statistical analysis he performed. Materials for this project were donated by Bisco (Schaumburg, IL) and GC America (Alsip, IL).
©Based on materials from the scientific and practical journal “Clinical Endodontics”: volume II, No. 1-2, 2008
Definitions
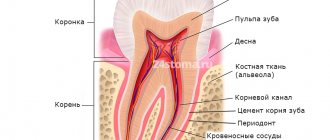
Tertiary dentin - dentin formed in response to an external stimulus (for example, caries). There are two types: reactive and reparative dentin.
Reactive dentin is formed by odontoblasts in response to an external stimulus (caries). Reparative dentin is formed by odontoblast-like cells in cases where deep caries is close to the pulp and odontoblasts have already been destroyed. Reparative dentin atubular.
Infected dentin is the outer layer of carious dentin that is infected with bacteria. Uninfected dentin is the inner layer of carious dentin that is demineralized but not infected by bacteria.
Indirect pulp capping is a treatment method that preserves the vitality of the dental pulp, where the deepest decay is left untouched to avoid accidental exposure of the pulp and the tooth is then restored taking into account the prevention of microleakages.