This video demonstrates a variant of the crown down root canal treatment technique (from the crown down), called the simplified anatomic technique by the author. The technique was developed by Professor Andre Machado, Brazil; the performer is one of his students.
The technique involves the absence of pressure (pressureless) and is recommended for curved canals. According to the author of the video, one of the advantages of this technique is the successful combination of low cost of its use and high efficiency.
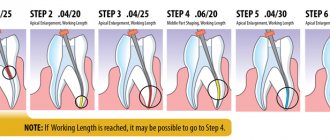
The technique includes five steps.
- Pulp removal (with a “carpet path”).
- Formation of the coronal and middle thirds.
- Snapshot to determine the full working depth of the tool.
- Formation of the apical third of the canal.
- Final irrigation (not shown in this video).
The video shows all 27 steps and is almost 11 minutes long. If desired, you can “skip” a step when its essence becomes clear. Below is the protocol in text, and at the very end of the article is a short English-Russian glossary of terms used in the video. For those who want to improve their “dental English”.
Subscribe to the YouTube channel Stomanet.ru!
[yuzo_related]
Pulp removal
- Pulp removal. File No. 15 H, 16 mm, filling motion.
- Irrigation.
- Pulp removal. File No. 10 K 18 mm, reciprocating twisting movements (as when winding a watch), alternating with pulling.
- Irrigation.
- Pulp removal. File No. 10 K 20 mm, reciprocating twisting movements (as when winding a watch), alternating with pulling.
- Irrigation.
- Pulp removal. File No. 08 K 22 mm, reciprocating twisting movements (as when winding a watch), alternating with pulling.
- Irrigation.
- Pulp removal. File No. 06 K 24 mm, reciprocating twisting movements (as when winding a watch), alternating with pulling.
- Irrigation.
- "Carpet". File No. 08 K 24, vertical reciprocating movements (up and down)
- "Carpet". File No. 10 K 24, reciprocating movements vertically (up and down)
- Irrigation.
- "Carpet". File No. 15 FF 24, reciprocating movements vertically (up and down).
Publications in the media
Down syndrome (trisomy 21, trisomy G) is a chromosomal disease caused by trisomy in the chromosome. 21, usually due to a violation of chromosome segregation during meiosis of the egg.
The frequency is 1 in 650 live births (the overall frequency in the population is higher, given that over 2/3 of affected fetuses die in utero). The frequency increases with maternal age, which is confirmed by amniocentesis data (especially sharply after 30 years).
Genetic aspects • Trisomy 21: 90-95% of patients have extra chr in all cells. 21 • Unbalanced translocation 21: 5% of patients have long arm chr. 21 is translocated to another chromosome, usually to 14. Among translocation trisomies, 1/2 are new, 1/2 are a consequence of a balanced translocation in one of the parents • Mosaic trisomy 21: 2 or more cell populations are found in 1–5% of patients : usually normal and trisomy 21 (clinical manifestations are usually less pronounced).
Pathomorphology. After 20 years, 100% of patients have plaques characteristic of Alzheimer's disease in the brain.
Clinical picture • Newborns and children •• Brachycephaly (100%) •• Mongoloid eye shape (90%) •• Epicanthus (90%) •• Muscular hypotonia (80%) •• Macroglossia (75%) •• Brushfield spots (light spots ["salt and pepper"] of the iris) on the iris (50%) •• Ear abnormalities •• Convergent strabismus •• Wide bridge of the nose •• Small chin •• Short neck •• CHD (up to 30% of children) •• Dermatoglyphics • •• Four-digit palmar fold ••• Absence of plantar curls (pads of the toes) ••• Convergence (up to fusion) of 2–3 flexor folds of the little finger •• Stenosis or atresia of the duodenum •• Absence of the anus •• Hirschsprung's disease in 2– 3% of children •• Delayed psychomotor development (may not appear until 1 year of age) •• Increased susceptibility to infections • Adults. Most manifestations are milder, brachycephaly persists. Patients experience delayed cognitive function (IQ - 40–45), although individuality and communication skills are preserved. After age 35, dementia similar to Alzheimer's disease develops. Most patients are capable of self-care. Some have jobs, although they require guardianship. Some patients exhibit autistic tendencies, and a small percentage of patients are nonverbal. Men are always infertile (no spermatogenesis).
Diagnostics • Study of the chromosome set (karyotype) is always necessary to exclude translocations • Given the frequent combination with leukemia - hematological studies annually • Determination of the level of thyroid hormones (hypo-, hyperthyroidism) is indicated • In children with pyuria and fever of unknown etiology - abdominal ultrasound to detect urinary tract abnormalities • In all children - EchoCG (VSD may not be apparent at birth).
Prenatal diagnosis • Ultrasound: •• Brachycephaly •• Hypotelorism •• Excessive cervical fold (16–29 weeks of gestation) •• Increased anteroposterior size of the nuchal space (10–14 weeks of gestation) •• Moderate ventriculomegaly •• CHD •• Hyperechoic intestine •• Duodenal atresia •• Non-immune hydrops fetalis •• Moderate hydronephrosis •• Shortening of the limbs •• Hypoplasia of the middle phalanx of the little finger • Biochemical parameters of maternal serum •• Decrease in the level of serum AFP less than 50% •• Increase in the level of hCG and unconjugated estriol.
Differential diagnosis. Trisomy 22 and deletion of the short arm of the chr. 9 may clinically resemble Down syndrome, which requires mandatory karyotype testing.
Management tactics • Genetic research and consultation • CVS research.
Surgery. Correction of congenital heart disease.
Complications • Intestinal obstruction (fistulas, intestinal tube abnormalities in 10% of cases) • Thyroid diseases (hypo- and hyperthyroidism in 5–8%) • Leukemia (0.5%) • Alzheimer's disease in older age.
Course and prognosis. The outcome and duration of the disease largely depend on the presence of congenital heart disease. Life expectancy is reduced: 30% die in the first year of life, 50% do not survive beyond the age of 5, and only 8% survive beyond 40 years. In 1/3 of patients, development is within normal limits in the first year of life; subsequently, mild deviations occur (slow development after the first year of life, moderate deviations in speech and cognitive functions). Gastrointestinal complications and heart failure with congenital heart disease can begin suddenly. Hypothyroidism usually appears 6 months after birth; a typical symptom is growth retardation.
Age characteristics. In 1/3 of patients over 35 years of age, clinical manifestations of Alzheimer's disease are observed.
Prevention • Prenatal karyotyping in women at risk • Low levels of AFP in maternal serum at 14–16 weeks of pregnancy (helps identify 1/3 of cases).
ICD-10 • Q90 Down syndrome
Note. The terms “Mongolism” and “Mongoloid idiocy” were previously used to refer to the disease.
Formation of the apical third of the canal
- Irrigation.
- Formation of the apical third of the canal. File No. 35 FF, 20 mm, reciprocating twisting movements (as when winding a watch), alternating with pulling.
- Irrigation. Passing the file 10 K, movements - as when removing pulp.
- Formation of the apical third of the canal. File No. 30 FF, 22 mm, reciprocating twisting movements (as when winding a watch), alternating with pulling.
- Irrigation. Passing the file 10 K, movements - as when removing pulp.
- Formation of the apical third of the canal. File No. 25 FF, 24 mm (passing), reciprocating twisting movements (as when winding a watch), alternating with pulling.
- Irrigation. Passing the file 10 K, movements - as when removing pulp.
Show your patients how their teeth work. This will help them understand you better and appreciate the treatment you provide more. The posters “Anatomy of a tooth blueprint”, “Anatomy of a tooth light” and “How a tooth works” will help you in this matter:
Stylish, light and bright. Choose:
https://lavka.stomanet.ru/product/stomatologicheskie-plakaty-anatomiya-zuba-blyuprint-a2/
https://lavka.stomanet.ru/product/stomatologicheskie-plakaty-anatomiya-zuba-lajt-a2/
https://lavka.stomanet.ru/product/stomatologicheskij-plakat-kak-ustroen-zub-a2/
Advantages and disadvantages of the technique
With a large number of advantages of coronal-apical processing methods, the inability to determine the length of the canal is a significant drawback.
Coronal-apical processing methods have the following advantages:
- Allows you to reach the farthest part of the tubule
- Gradual removal of waste particles reduces the risk of intracanal infection
- It is easy to inject medicine into the resulting depression
- The risk of the tool getting stuck inside the tooth is minimized
- The risk of blocking the far part of the canal with dentin particles and destroyed soft tissues is minimal
- The method allows not to reduce the working depth
- The natural shape of the root canal is not disturbed
The main disadvantage of the technique is that the doctor cannot determine in advance how long the canal is and how clogged it is. Therefore, it takes him quite a lot of time and effort to process the withdrawal.
Learning Dental English
Coronal third, middle third, apical third
– coronal third, middle third, apical third (tooth root).
Glide path
– “carpet path”, a processed section of the canal that makes it easier.
Working length
– working length (for example, endotool).
Mesiobuccal
– medial buccal (about the root); mesial - medial, buccal - buccal.
GG drill
– Gates-Glidden drill
Patency
– channel passage
“Crown Down” technique (from the crown down)
The “Crown Down” technique involves staged processing of the canal from the mouth to the apex with a sequential change of instruments from larger to smaller sizes. In this case, parietal dentin is removed only by the apical part of the instrument, which improves tactile control and reduces the risk of jamming and fracture of the instrument (Fig. 152).
Mechanical treatment of the canal in accordance with the “Crown Down” technique is carried out as follows.
The first stage is the introduction of a K-file No. 35 into the root canal to a depth of 16 mm.
First, they try to insert a K-file No. 35 according to ISO into the root canal to a depth of 16 mm (Fig. 152a).
If it is not possible to insert this file to such a depth, an x-ray of the tooth is taken with the instrument inserted into the canal. The purpose of this operation is to find out what caused the instrument to get stuck: curvature of the root canal or narrowing of its lumen.
If the reason is a narrowing of the root canal, then it is expanded with thinner K-files to a depth of 16 mm until a K-file No. 35 is inserted at 16 mm (Fig. 1526, c, d, e, f).
If the reason for the stuck K-file No. 35 is curvature of the root canal, then the canal is processed to the area of curvature.
If the K-file was immediately inserted into the canal 16 mm or more, mechanical treatment of this part of the canal is performed.
The second stage is the determination of the “temporary working length”.
For this purpose, a “measuring” radiograph is taken with a K-file in the canal, which is approximately 3 mm short of the physiological apex. The length of the channel is calculated. The indicator assigned when analyzing such a radiograph is called the “temporary working length”.
To determine the “temporary working length,” a diagnostic radiograph can also be used if it was taken at the first stage of instrumentation of the canal.
The third stage is the passage of the apical part of the canal to the “temporary working length”.
This stage begins by inserting a K-file No. 35 into the canal until it stops, then, without apical pressure, make two full turns of the instrument clockwise and remove it from the canal (Fig. 152g). Next, take a K-file No. 30, insert it into the canal as far as it will go and rotate it clockwise without pressure until maximum movement in the apical direction and remove it from the canal (Fig. 152h). Then a similar operation is carried out with K-file No. 25, then No. 20, etc. until the “temporary working length” is reached (in our case - up to No. 25 (Fig. 152i)). The fourth stage is determining the “final working length”. A “measuring” radiograph is taken with the endodontic instrument inserted into the canal to a “temporary working length”. The “final working length” is determined. The fifth stage is expansion of the root canal.
This stage begins by inserting a K-file No. 40 into the canal until it stops, then without apical pressure, make two full turns clockwise and remove the file from the canal (Fig. 152k). Next, take a K-file No. 35, insert it into the canal all the way and rotate it clockwise without pressure until the instrument moves maximum in the apical direction and remove it from the canal (Fig. 152l). Then a similar operation is carried out with K-file No. 30, then No. 25, No. 20, No. 15, etc. until the working length is reached (in our case - up to No. 30 (Fig. 152m)).
After this, the same manipulations are repeated, starting with K-file No. 45 (Fig. 152n, o, p), then with No. 50 (Fig. 152p, s, t). Each time they strive for deeper penetration of files.
Mechanical treatment of the canal is continued until its apical part is expanded to the desired diameter, but not less than to No. 25 (in our case, to No. 40 (Fig. 152t)).
Using the “Crown Down” technique allows you to maintain the original shape and direction of the channel, however, this method is quite labor-intensive. Therefore, it is most often used when expanding root canals using machine tools: profiles or GT files.
In conclusion, we would like to dwell on one more question: “To what diameter should the root canal be expanded?”, because the diameter corresponding to ISO No. 25 is the minimum, which provides only more or less acceptable conditions for filling the canal, while
| Table 43. Recommended dimensions of mechanical expansion of the apical part of the canal (Kerekes K., Tronstad L. /1977/) Teeth of the upper jaw Recommended expansion of the apical part of the canal 1 70-90 2 60-80 3 50-70 4 (two roots) 35-70 5 60-90 6i7 anterior buccal canal 35-60 posterior buccal canal 40-60 palatal canal 80-100 Mandibular teeth Recommended expansion of the apical part of the canal 1 and 2 45-70 3 50-70 4 and 5 50-70 6i7 anterior canals 35 -45 rear channel 60-80 |
however, neither the thickness of the root, nor the possibility of effective drug treatment, nor the degree of canal curvature are taken into account.
7. Assignment for independent work on the topic being studied:
1. List the stages of root canal formation using the Crown Down technique and indicate the purpose of each stage.
2. Specify the sequence of use of endodontic instruments when performing the “Crown Down” technique
3. Schematically represent instruments with aggressive and non-aggressive tips.
Recommended reading: