basic information
Syphilis is an infection that can be transmitted between people in various ways and poses a direct threat to life. Foci of syphilis can be located in intimate areas, on the arms, and torso. In recent years, cases of infection in the mouth have become more frequent. The following photos in the new collection of the site Obolezi.com will demonstrate what it looks like.
Manifestations of syphilis in the mouth in the secondary period of the disease
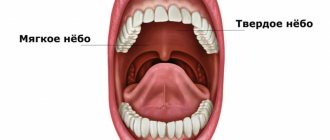
During the period of generalization of the infectious process in the secondary period of syphilis, secondary syphilides appear on the mucous membranes of the oral cavity - rashes in the form of roseolas and papules. The mucous membrane of the tongue, cheeks, soft palate, palatine arches, tonsils are the main places of their localization.
Syphilitic roseola in the oral cavity is localized on the tonsils and soft palate and appears as a bright red spot. When roseola merge, large areas of hyperemia are formed, sharply delimited from the surrounding tissues. The general health of the patients remains satisfactory.
Papular syphilides in the oral cavity (dense elements) have a round shape and dough-like consistency, they have a dense base and clear boundaries, they are bright red in color, painless. Constant irritation leads to the appearance of erosion papules on the surface. Papules are most often located on the mucous membrane of the gums, cheeks, along the edges and on the tip of the tongue, in the corners of the mouth, less often - on the mucous membrane of the nose, pharynx, hard palate, vocal cords, epiglottis and eyes.
- Erosive-ulcerative syphilides often appear on the soft palate and tonsils.
- Papules located in the corners of the mouth resemble jams.
- Papules located on the back of the tongue look like bright red, oval-shaped formations with a smooth surface - devoid of papillae (“mown meadow symptom”).
- Papules localized on the vocal cords lead to hoarseness and even complete loss of voice.
- Papular syphilide of the nasal mucosa occurs as a type of severe catarrhal inflammation.
Papules should be distinguished from bacterial tonsillitis, lichen planus, diphtheria, aphthous stomatitis, flat leukoplakia, etc.
Rashes in the oral cavity due to secondary syphilis are extremely contagious.
Pustular syphilide on the oral mucosa is rare. The developed infiltrate disintegrates, forming a painful ulcer covered with pus. The general condition of the patient suffers.
Rice. 3. Syphilis in the mouth - papular syphilide of the hard palate.
Risks of getting sick
If you are confident that your body is ready to withstand any challenge, know: after the first contact with a patient, the chances of being photographed showing syphilis on the face are 80%. The remaining 20% is not due to the presence of immunity to treponema, but to too little of it to cause a big problem.
Manifestations of syphilis in the mouth during the tertiary period of the disease
In 30% of cases during the period of tertiary syphilis, the mucous membranes of the nose, soft and hard palate, tongue and posterior pharyngeal wall are affected. Tertiary syphilides are always few in number, appear suddenly, there are no signs of acute inflammation and subjective sensations. There is often no response from the lymph nodes.
Gummous syphilide of the mucous membrane appears in the form of a small node, which, due to sudden infiltration and swelling, increases in size and acquires a dark red color. The boundaries of the gummous lesion are clear. Over time, the infiltrate disintegrates, soft tissue and bone formations are destroyed, which leads to irreversible deformations and impaired organ function.
The resulting ulcer is deep, has crater-shaped edges, congestive-red color, sharply demarcated from the surrounding tissues, painless, with granulations at the bottom. During healing, a retracted scar is formed.
- The disintegration of the gumma located on the hard palate leads to its perforation.
- The disintegration of the gumma located in the area of the nasal septum leads to its deformation (“saddle nose”) and perforation of the nasal septum, the integrity of the organ and the function of breathing, swallowing and phonation are disrupted. The resulting perforations do not close during healing.
The rashes of the tertiary period of syphilis are practically not contagious, since they contain a minimal number of pathogens.
Tuberous syphilide is less common. The tubercles most often appear on the lips, soft palate and uvula (vera palatine), hard palate and the mucous membrane of the upper jaw that supports the teeth (alveolar process). The tubercles are dense to the touch, small, prone to grouping, reddish-brown in color, and quickly disintegrate with the formation of deep ulcers. Healing occurs in scars.
Rice. 4. The photo shows the consequences of tertiary syphilis in the mouth - perforation of the hard palate.
More about symptoms
Symptoms vary depending on the current stage. So, at first, signs of infection appear only by the appearance of papules on the skin (or mucous membranes, in the case of a photo of syphilis in the throat), in place of which an ulcer later forms. By the end of the first stage, the ulcers disappear on their own and appear with renewed vigor in the second. With the beginning of the second stage, internal organs begin to suffer. At the third stage, total intoxication of the body occurs. The rash on the body becomes massively lumpy.
Manifestations of syphilis in the mouth during the primary period of the disease
With primary syphilis, ulcers appear at the site of pathogen penetration - hard chancre (hard ulcers, primary syphilomas). The reason for their occurrence in the mouth is the transmission of infection through sexual perversion, less often - kissing a patient, using infected dishes and personal hygiene items, wind instruments and smoking pipes. Hard chancroid can appear on the mucous membrane of the lips, tongue and tonsil, less often on the gums, mucous membrane of the hard and soft palate, pharynx and larynx.
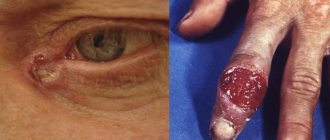
Hard chancre (primary syphiloma) forms 3 to 4 weeks after the initial infection. Its size is 1 - 2 cm in diameter. There is no pain or other subjective manifestations of the disease. Single erosive chancres are more common. They have a smooth shiny surface, bright red color, round or oval shape. The compaction at the base is less pronounced.
Hard ulcerative chancres are more common in individuals with severe concomitant diseases and reduced immunity. They have a deep defect in the center - an ulcer and pronounced compaction at the base. The bottom of such an ulcer is covered with a dirty yellow coating, and there is copious discharge. Often small hemorrhages form at the bottom.
Rice. 2. In the photo there is syphilis of the tongue in the primary period of the disease - chancre on its lateral surface.
Syphilis of the tonsils (syphilitic tonsillitis)
Treponema pallidums have a tropism for lymphoid tissue, which is why syphilitic tonsillitis and enlarged lymph nodes are recorded at all stages of the disease.
Syphilis of the tonsils in the primary period
During the period of primary syphilis, chancre is sometimes recorded on the tonsils. The disease occurs in several forms - anginal, erosive, ulcerative, pseudophlegmonous and gangrenous.
- In the anginal form of the disease, the primary chancre is often hidden in the submygdaloid sinus or behind the triangular fold. The patient's body temperature rises and moderate pain in the throat appears. The palatine tonsil is hyperemic and enlarged in size. Regional lymph nodes are enlarged.
- When an oval-shaped red erosion with rounded edges, covered with gray exudate, appears on the tonsil, they speak of an erosive form of tonsil chancre. The bottom of such erosion has a cartilaginous structure.
- In the ulcerative form, a round ulcer appears on the palatine tonsil. At its bottom there is a film that is gray in color (syphilitic diphtheroid). The disease occurs with high body temperature, sore throat radiating to the ear on the affected side, and increased salivation.
- The pseudophlegmonous form of the disease occurs as peritonsillar phlegmon. Massive doses of antibacterial drugs significantly improve the patient’s condition, but the syphilitic process continues.
- In the case of the addition of a fusospirile infection, a gangrenous form develops. The disease is characterized by the development of a septic process and gangrene of the tonsil.
A long course and lack of effect from symptomatic treatment are characteristic signs of primary syphilis of the tonsils - chancre-amygdalitis.
Rice. 11. In the photo there is syphilis of the tonsils - chancre-amygdalitis, ulcerative form.
Rice. 12. In the photo, the anginal form of the disease is chancre-amygdalitis of the right tonsil. A characteristic feature is the characteristic copper-red color of the tonsil and the absence of inflammation of the surrounding tissues.
Syphilitic tonsillitis of the secondary period of the disease
With secondary syphilis, secondary syphilides - roseola and papules - may appear on the soft palate, tonsils and arches.
- Roseola (spots of hyperemia) during the disease are located either isolated or can merge and form large areas of hyperemia. The lesion is called erythematous syphilitic tonsillitis. Roseolas are red in color and sharply demarcated from surrounding tissues. The patient's condition remains satisfactory.
- When papules appear on the tonsils and the area of the lymphoid ring, they speak of papular syphilitic tonsillitis . Papules merge to form plaques. The rashes have clear boundaries. With constant irritation, the papules become ulcerated and covered with a whitish coating, pain appears when swallowing, the temperature rises, and the general condition of the patient worsens.
Rice. 13. In the photo there is syphilis in the mouth. On the left is syphilitic erythematous tonsillitis, on the right is papular tonsillitis.
Rice. 14. The photo shows erythematous syphilitic tonsillitis.
Syphilis of the tonsils in the tertiary period of syphilis
In the tertiary period of syphilis, gumma may appear on the tonsil. The disintegration of gumma leads to complete destruction of the organ and surrounding tissues. Cicatricial deformation of the pharynx leads to the development of severe atrophic pharyngitis.
Consequences
The presence of chancre clearly indicates the presence of the causative agent of syphilis in the body. This disease in itself is very dangerous, as it can affect internal organs, causing their failure.
Also, the consequences of infection are destructive processes in bone tissue, which deprives a person of the ability to lead normal life activities and provokes physical deformities. Without treatment, the risk of developing neurosyphilis increases. Later, as the disease progresses, death occurs - this is the price of ignoring the problem.
If we consider directly the consequences associated with the formation of chancre, it is worth highlighting the following:
- damage to deep tissue layers;
- suppuration and tissue necrosis;
- self-amputation of damaged areas, in particular the external genitalia;
- bleeding;
- formation of rough scars;
- urethral perforation;
- accession of infections;
- endocervitis of the cervix;
- balanoposthitis;
- syphilitic gangrene;
- bartholinitis.
Such complications occur mainly with atypical syphilomas. Common chancre often goes unnoticed and disappears without a trace as the disease moves into the secondary phase.
Treatment methods
The sooner treatment is started, the better for the patient. Instructions for taking medications are drawn up on an individual basis, depending on the nature of the disease and the characteristics of the patient’s body.
The main therapeutic drugs used are:
- penicillin antibiotics;
- fluoroquinolones;
- tetracyclines;
- macrolites;
- immunostimulants;
- probiotics;
- vitamin complexes;
- antimycotics;
- bismuth preparations;
- iodine preparations.
If syphiloma is detected in the mouth, rinsing with solutions of boric acid, furatsilin, gramidicin is prescribed. It is imperative to observe hygiene standards to prevent secondary infections.
Sexual partners of an infected person with whom he has had contact in the last few months require preventive treatment and constant monitoring. Until stable remission occurs, you should not stop taking medications without obvious reasons, or enter into intimate relationships. We also recommend watching the video in this article to learn more about syphilitic chancre.
Syphilis of the soft palate
The soft palate (vera palatine) is often affected along with the hard palate in tertiary syphilis. Gummas may appear on it, but gummatous infiltration occurs more often. The affected areas have a rich purple color and lead to stiffness of the soft palate. As a result of cicatricial changes, atresia (fusion) of the pharynx occurs. The soft palate fuses to the back of the oropharynx, causing the oral and nasal cavities to separate. Organ function is impaired.
With the development of tubercular syphilide, isolated elements are formed on the soft palate, the breakdown of which forms ulcers that heal with scars. Scar tissue leads to deformation of the organ.
Rice. 19. Damage to the soft palate (schematic representation).
Syphilis of the hard palate
With primary, secondary and tertiary syphilis, the hard palate can be affected. Gummas of the hard palate can affect not only the mucous membrane, but also spread to the bone structures of the organ, which leads to their destruction and perforation.
Syphilis of the hard palate in the primary period of the disease
Primary syphiloma (chancroid) on the hard palate appears 3 to 4 weeks after infection. With ulcerative chancre, a hard infiltrate is located at the base. In the case of the formation of a deep ulcer, the infiltrate at the base acquires a cartilage-like structure. With erosive chancre, the infiltrate at the base is barely noticeable and weakly expressed. Even without treatment, after 4 to 8 weeks, the ulcer and erosion scars on its own. Scarring occurs much faster under the influence of specific treatment.
Rice. 15. Syphilis in the mouth. Primary syphiloma of the hard palate.
Syphilis of the hard palate in the secondary period of the disease
With secondary syphilis, papular syphilides more often appear on the mucous membrane of the hard palate. They are dense, flat, round, smooth, red, located on a dense base, with clear boundaries, painless. Frequent irritation leads to the appearance of areas of maceration on the surface, and sometimes papillary growths. As papules grow, they merge.
Rice. 16. Syphilis in the mouth - papules on the hard palate and tongue (photo on the left) and papules on the hard palate (photo on the right).
Syphilis of the hard palate in the tertiary period of the disease
When gumma is located on the hard palate, the disease is tragic. Due to the thin mucous membrane, the gummous process quickly spreads to the periosteum and bone. When gumma disintegrates, the bone quickly becomes necrotic and sequestra (dead areas) appear. As a result of perforation, a communication occurs between the nasal cavity and the mouth, which leads to difficulty eating and speech impairment.
Rice. 17. Gummous infiltration of the hard palate (photo on the left) and gummous infiltration (photo on the right).
Rice. 18. The photo shows the consequences of tertiary syphilis - perforation of the hard palate.
Diagnostics
To carry out successful treatment, it is important to detect syphilis chancre in time and begin treatment of the disease. Before prescribing drug therapy, it is necessary to verify the correctness of the diagnosis, since the possibility of false suspicions cannot be excluded.
The following types of studies can be used for diagnosis:
- ELISA;
- Wasserman reaction;
- microprecipitation reaction;
- RIBT;
- REEF;
- passive hemagglutination reaction;
- serological tests.
Syphilis is confirmed by the presence of treponema pallidum in tissue scrapings, as well as antibodies to it in blood samples. Based on the results of tests and physical examination, one can judge the extent of the infection.
It is also necessary to carry out a differential diagnosis of the following diseases (depending on the location of the chancre and the presence of accompanying symptoms):
- angina;
- herpes;
- candidiasis;
- tuberculosis;
- traumatic erosions.
Syphilis of the tongue in the tertiary period of the disease
In the tertiary period of syphilis, single or multiple gummas (nodular glossitis) more often appear on the tongue, diffuse (spread) sclerosing glossitis develops less often. Sometimes, isolated gummas appear against the background of sclerosing glossitis.
The gummous infiltrate is large in size (about the size of a walnut), quickly disintegrates with the formation of a deep ulcer and an uneven bottom, surrounded by a shaft of dense infiltrate. The developed scar tissue significantly deforms the tongue.
Sclerosing glossitis is characterized by the development of diffuse infiltration in the thickness of the tongue. The tongue becomes dense, acquires a dark red color, and the mucous membrane thickens. As a result of rapidly developing sclerosis, when muscle fibers are replaced by dense connective tissue, the tongue contracts and becomes smaller in size, its surface is smoothed (loses papillae), becomes bumpy, and becomes significantly denser (“wooden” tongue). There is increased salivation (salivation). Appearing cracks often become infected, which leads to the appearance of erosions and ulcers that are prone to malignancy. The disease occurs with severe pain, the patient's speech is impaired and eating is difficult.
Rice. 10. Syphilis of the tongue in the tertiary (late) period of the disease - a single gumma of the tongue (photo on the left) and a disintegrating gumma (photo on the right).
Causes and course of the disease
The development of syphilis of the pharynx is possible at all 3 stages of the disease.
Primary lesions are more often in the nasopharynx than in the oropharynx. Moreover, infection can also occur through the use of infected medical instruments (iatrogenic factor of infection).
When the nasopharynx is affected, the most common manifestations of the disease are:
- Enlargement of the lymph nodes of the neck, which in some cases are very pronounced;
- Severe pain when swallowing, which radiates to the ear and is accompanied by congestion.
Syphilis of the throat: damage to the pharynx
The pharynx is the initial part of the digestive tract and respiratory tract. It connects the nasal cavity and the larynx, the vocal organ.
Damage to the pharynx in primary syphilis
With primary syphilis, unilateral lesions are more often observed. Chancre can be erythematous, erosive or ulcerative. Treponema pallidum has a tropism for lymphoid formations of the throat. Their defeat leads to the appearance of an indomitable cough. With the disease, regional lymph nodes always enlarge.
Damage to the pharynx with secondary syphilis
The pharynx in secondary syphilis is often affected along with the larynx. At the same time, skin rashes appear on the patient’s skin—secondary syphilides.
Damage to the pharynx in tertiary syphilis
In tertiary syphilis, damage to the pharynx occurs in the gummous form, diffuse and early ulcerative-serpentiform forms.
- The gummous infiltrate does not manifest itself in anything until ulceration appears. When gumma disintegrates, bleeding may occur and the bones of the spine and skull may be destroyed. As a result of the development of scar tissue, communication (partially or completely) between the nasal and oral cavities is disrupted. Breathing becomes possible only through the mouth, the voice changes, taste and smell disappear.
- In the diffuse syphilomatous form, multiple lesions are observed on the mucous membrane of the pharynx. At the beginning of the disease, the changes are in the nature of hypertrophic pharyngitis. But then an extensive syphilitic ulcer is formed, similar to carcinoma.
Syphilis on the tongue
The tongue with syphilis is affected in the primary, secondary and tertiary periods of the disease.
Syphilis of the tongue in the primary period of the disease
Hard chancre on the tongue is often single, ulcerative or erosive in nature. Sometimes it has a slit-like shape located along the tongue.
Rice. 5. Syphilis of the tongue in the primary period - chancre. Syphilide is an erosion or ulcer with a dense infiltrate at the base.
Rice. 6. The photo shows a hard chancre on the tip of the tongue.
Syphilis of the throat: damage to the larynx
The larynx is the upper part of the respiratory system and the organ of voice production. It is located in the front of the neck, where the Adam's apple (thyroid cartilage) is formed.
Damage to the larynx in secondary syphilis
With secondary syphilis, the appearance of roseola or papular rashes on the vocal cords is noted, which leads to syphilitic dysphonia (violation of the sound of the voice) or aphonia (complete absence of voice). Diffuse erythema is similar to catarrhal laryngitis. Since secondary syphilides in the larynx do not show themselves for a long time, the disease goes unnoticed at first, and the patient all this time poses a danger to others.
Damage to the larynx in tertiary syphilis
- During the period of tertiary syphilis, gummas may appear in the larynx. When they disintegrate and a secondary infection occurs, inflammatory swelling appears, which leads to difficulty breathing. The ulcer, when the gumma disintegrates, has crater-shaped, sharply defined edges, is dense, with a greasy bottom. When the gumma is located on the epiglottis, the presence of a foreign object in the throat is felt. With large infiltrate sizes, laryngeal stenosis develops. Scarring of syphilitic ulcers located on the vocal folds and when the arytenoid cartilages are damaged, the voice becomes hoarse forever, sometimes aphonia develops (complete loss of sonority of the voice). Soreness is often absent or insignificant.
- With the development of a diffuse gummous infiltrate, the lesion affects the superficial layers of the organ, sometimes deep, when the pathological process passes to the muscle layer and perichondrium. The site of infiltration has the appearance of reddish-yellow thickenings with an inflammatory rim along the periphery, often extending to the epiglottis, or ligamentous apparatus, or subglottic region. With ulceration, the surface of the diffuse gummous infiltrate becomes uneven.