Pain in the throat and ear is a clinical manifestation of a number of otolaryngological diseases, and much less often - neoplasms of a malignant nature. Most often it is one-sided and signals the presence of inflammatory processes occurring in the sinuses, tonsils, lymph nodes and larynx. Treatment of chronic sore throat is aimed at eliminating inflammatory processes and pain symptoms. For this, the otolaryngologist prescribes medications.
The otolaryngology department of CELT offers diagnosis and treatment of chronic ear pain. Our multidisciplinary clinic has been operating in the paid medical services market in Moscow for almost thirty years. Our specialists operate with international treatment standards and have everything necessary for accurate diagnosis and effective treatment in accordance with them.
At CELT you can consult an otorhinolaryngologist.
- Initial consultation – 3,000
- Repeated consultation – 2,000
Make an appointment
Anatomy of the throat
In the pharynx and larynx, as well as at the border of the oral and nasal cavities along the back wall of the pharynx, there are accumulations of lymphoid tissue - the lymphoid-pharyngeal ring. It performs a protective function and is an important organ of our immunity. The largest collections of lymphoid tissue are called tonsils and there are several of them: two palatine, two tubal, one pharyngeal (aka adenoid) and one lingual.
Below is the larynx - this is a complex organ, representing a complex of various tissue structures, consisting of several cartilages, muscles, with a developed network of blood, lymphatic vessels and nerves.
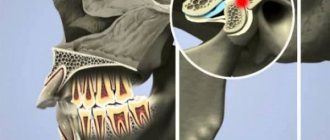
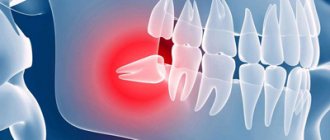
Causes of temporomandibular joint arthritis
Arthritis does not show pronounced symptoms immediately; its development can be asymptomatic for a long time or with minor pain. Out of habit, a person reacts to pain by taking painkillers, which only makes the situation worse. Anesthetics relieve symptoms, but do not remove the cause. The disease “takes over” more and more healthy tissue and, as a result, instead of treatment, the patient receives disability. Let's figure out why TMJ arthritis can develop.
- 1. Mechanical injury. Impact, the habit of clenching teeth tightly, and active chewing of hard food can lead to damage to one or more components of the joint. Articular tissues respond to damage with pain and dilation of blood vessels. Simply put, blood enters from the vessels directly into the tissue, causing swelling, inflammation, and, if treatment is delayed, suppuration.
- 2. Infection. The inflammatory process develops as a result of pathogenic microorganisms entering the joint through the blood or through direct and contact routes. The direct route of infection involves inflammation of the TMJ as a result of an open wound (knife or gunshot wound). If microorganisms have penetrated into the cartilage from infected muscle or bone tissues, then the pathology of transmission is called contact. All diseases of the oral cavity (as well as ear, nose and throat) can lead to arthritis of the temporomandibular joint through the hematogenous route, through the blood.
- 3. Systemic inflammation. Some pathologies of an inflammatory nature (herpes, hepatitis, mycoplasmosis, chlamydia, lupus), if not treated in a timely manner, affect connective tissue throughout the body.
Main causes of sore throat
- viral infections - ARVI and influenza, enterovirus, Epstein-Barr virus, Coxsackie virus (acute pharyngitis, acute tonsillitis)
- bacterial infections (acute tonsillitis caused by streptococci, staphylococci, diphtheria)
- fungal infections (candidiasis of the oral cavity, pharynx or larynx)
- thermal and chemical burns
- gastroesophageal reflux (GERD)
- trauma and foreign body entry
- strong voice load
- complications of pharynx diseases (peritonsillitis, peritonsillar abscess, phlegmon)
- some diseases of the ENT organs, which may be accompanied by a sore throat (acute sinusitis, acute laryngitis)
- the presence of various tumors in the throat, benign and malignant
- allergic reactions, Quincke's edema
- chronic diseases of the pharynx (chronic tonsillitis, chronic pharyngitis, chronic laryngitis)
- also the throat may be red due to various dyes
Most often, a sore throat worries patients with ARVI.1
Causes of pain under the jaw
There are many reasons for pain in the neck and/or jaw, and they can indicate various health problems. There are many structures in the neck area, the pathologies of which cause pain and serious discomfort.
Pathological changes in lymph nodes
There are many lymph nodes behind our ears, on our neck, and in the lower part of our jaw. And one of the diseases that leads to painful discomfort is called lymphadenitis. This is inflammation of the lymph nodes due to bacterial or other infections. It is accompanied by severe sharp pain in the neck, which will radiate to the jaw, and will also cause an increase in body temperature. Without treatment, lymphadenitis becomes chronic, and then constant fatigue, weight loss and general malaise are added to the elevated temperature. Another pathology may be tumors that appear on the lymph nodes. These are, as a rule, metastases that have penetrated from any organs affected by cancer. The nature of the pain varies, but weakness and weight loss also accompany this condition.
Glossitis
Another disease that is associated with an inflammatory process, but does not affect the lymph nodes, but the tongue. Signs of glossitis are a bright red color of the tongue, severe swelling of the tongue and lower jaw. There may also be purulent discharge from the glands in the mouth, pain radiating to the ear, jaw and neck.
Pharyngitis, tonsillitis, sore throat
These diseases can also cause pain. But at the same time, if your neck hurts, then the pain radiates not under the jaw, but into the throat. With a sore throat, the pain intensifies at the time of swallowing, and the person also develops all the signs of an acute respiratory infection or flu (ear pain, fever, weakness, lack of appetite, etc.). For acute pharyngitis
Possible inflammation of the lymph nodes.
Jaw fractures
A fracture in the lower part of the jaw occurs due to a strong blow, head injury or accident. Fractures can be direct or reflected, multiple, fragmented, displaced, open or closed, but in any case the person experiences severe pain, which is accompanied by swelling, hemorrhage and impaired chewing function. In case of a fracture, you should immediately consult a doctor.
Diagnosis of sore throat
If the patient is bothered by a sore throat, then it is necessary to contact an ENT doctor as soon as possible. Untimely or incorrect treatment can lead to the development of a chronic course of the disease.
The doctor will conduct a detailed survey about how long your throat has been hurting, what other symptoms are bothering you, whether you have undergone any independent treatment, and so on. A detailed medical history must be collected in order to determine the cause of a sore throat, make a correct diagnosis and prescribe effective treatment.
The doctor conducts a thorough examination of the throat and may examine the larynx.
Diagnostic methods:
- pharyngoscopy is an examination of all parts of the pharynx visually and with the help of special instruments that allow you to carefully examine the pharynx and nasopharynx
- laryngoscopy is an examination of the larynx with a special mirror
- endoscopic examination - examination of the pharynx and larynx using special endoscopic equipment (fiberoscopy)
- computed tomography (CT), if necessary with contrast
- Magnetic resonance imaging (MRI) is performed for soft tissue pathologies
Depending on the cause of the disease, the patient may be sent for consultation to doctors of other specialties, such as a gastroenterologist, neurologist, oncologist, dentist, and others.
The doctor may prescribe various additional laboratory tests (complete blood count, ESR, C-reactive protein, flesh culture, etc.).
Types of neck and jaw pain
The neck may hurt on the left side under the jaw, or the pain occurs on the right or in the front and radiates to the back. The nature of pain can be very different, due to one or another reason for its occurrence. The nature of the pain is very important for making a diagnosis, so it is necessary to describe it to the doctor as accurately as possible.
Intense pain on the sides of the neck under the jaw
Most often, such pain occurs due to inflammation of the lymph nodes and tonsillitis. Both diseases are the result of an infection entering the body. Migraines and dental infections can also cause severe pain under the jaw.
It's a dull pain
If the pain is aching in nature, then it could be caused by a migraine, which, with bright light, changes in lighting or loud sounds, intensifies and concentrates in one place. Additionally, symptoms such as vomiting, nausea, vision problems and constant thirst may appear. Aching pain can also be associated with infectious dental diseases.
Pain under the jaw on the left
If your neck hurts on the left side under the jaw, then this may indicate almost any of the diseases that were listed above; Pain can also be associated with problems in the cardiovascular system. For example, pain on the left under the jaw appears with a heart attack or angina, which, as a rule, comes from pain in the chest area and is accompanied by acute pain in the teeth.
Pain when pressing
If your neck under your jaw begins to hurt when pressed or pressed, this may indicate inflammation of the lymph nodes, as well as diseases such as auricular ganglion neuralgia, osteogenic sarcoma, or the presence of sialoliths. Any painful sensations cannot be ignored. Even if discomfort in the neck and jaw does not cause any particular problems, this is not a reason to ignore it. Seeing a doctor in a timely manner is a decision that needs to be made immediately. Only a doctor can tell why your neck hurts under your jaw and what needs to be done about it.
Treatment for sore throat
Treatment depends primarily on the cause of the sore throat.
Therapy may include:
- antibiotics, antifungals or antivirals to eliminate the pathogen
- anti-inflammatory, antiseptic drugs for topical use and anesthetics to relieve sore throat. Local therapy in the form of rinses, sprays, various tablets and lozenges for resorption Tantum® Verde
- taking antipyretic medications if necessary
- rinsing with a solution of calendula or chamomile
- gentle diet
- physiotherapeutic methods – UHF therapy, quartz, electrophoresis
- surgical treatment to remove foreign bodies, injuries or various tumors
- consultation with other specialists
Chronic tonsillitis and related diseases
A. Yu. Ovchinnikov, A. N. Slavsky, I. S. Fetisov
Department of Otorhinolaryngology MMA named after. I. M. Sechenova
Currently, about 100 different diseases are known, largely due to chronic tonsillitis. The lack of a therapeutic effect or short-term remission in such diseases is often due to the fact that doctors do not take into account the pathology of the pharynx as a possible cause that provokes and maintains associated painful conditions in other organs and systems of the body.
The purpose of this publication is to draw the attention of practitioners to a fairly large number of diseases that develop against the background of pharyngeal pathology, but are often not considered in the context of this relationship. The changes in internal organs are most pronounced in the decompensated form of chronic tonsillitis. They are caused by the influence of neuro-reflex, bacteremic, toxicemic and allergic factors.
An imbalance in the immune status is also determined - redistribution in the content of T- and B-lymphocytes and their subpopulations, the presence of circulating immune complexes, sensitization of granulocytes to bacterial allergens.
Circulating antigen-antibody immune complexes have chemotoxic activity and increase the proteolytic ability of macrophage enzymes, which leads to lysis of tonsil tissue and denaturation of tissue proteins, which as a result acquire antigenic properties. Once in the blood, they cause the formation of autoantibodies. Thus, the palatine tonsils become a site of permanent delayed-type sensitization to the antigens of streptococcus and staphylococcus - microflora that most often grows in the lacunae of the palatine tonsils.
The neuro-reflex mechanism of the influence of chronic tonsillitis on the formation of associated pathology is also described. A.M. Monaenkov was the first to discover and study the afferent connections of the palatine tonsils with the most important subcortical formations, in particular with the co-structures of the posterior section of the subtubercular region of the hypothalamus. It is these nerve structures that are involved in the regulation of natural active immunity, which determines the central determination of disturbances in immunological reactivity in chronic tonsillitis.
It has been established that under the influence of the flow of afferent signals from the tonsillar region, the functional state of the nuclei of the subthalamic region is disrupted and adrenergic receptors of neurons are excited. This serves as a trigger for the development of disruption of autonomic synergism and subsequent chain disorganization of other nervous structures. Such disturbances of neurodynamic processes in certain subcortical and cortical parts of the brain are called a “tonsillogenic” neurodystrophic process and are assessed as an obligatory component in the pathogenesis of any metatonsillar lesions.
It is also possible to have a toxic effect on the body during chronic inflammation of the tonsils due to the dissemination of toxins by the hematogenous or lymphogenous route.
It is now known that, along with the well-studied and thoroughly described influence of chronic tonsillitis on the formation of pathology of the heart, joints and kidneys, there are a large number of other associated painful manifestations. Thus, chronic tonsillitis creates real preconditions for the development of dermatoses. This, in particular, is confirmed by the rather high frequency of detection of chronic tonsillitis in patients with psoriasis and the presence in them of a clear relationship between the activity of the clinical course of this disease and the exacerbation of chronic tonsillitis. Many researchers consider tonsillectomy one of the most important components of treatment for patients with psoriasis. Sanitation of the focus of chronic infection normalizes altered reactivity and reduces allergenicity of the body, eliminates the pathological reflex effect on the central nervous system. It is advisable to perform tonsillectomy in the earliest stages of development of dermatosis. Conservative treatment should not be abandoned, since isolated cases of exacerbation of psoriasis after tonsillectomy have been described. A positive result is manifested in stable remission or mitigation of the clinical picture of exacerbations.
Neurodermatitis is often combined with chronic tonsillitis, which in this case quickly becomes widespread with frequent relapses complicated by pyoderma.
Treatment of neurodermatitis without sanitation of the source of chronic infection is ineffective.
Chronic tonsillitis plays a role in the occurrence and course of collagen diseases (systemic lupus erythematosus, scleroderma, hemorrhagic vasculitis, periarthritis nodosa, dermatomyositis, polyarthritis). A similar antigenic structure of some collagenoses and chronic tonsillitis has been proven; for example, hemorrhagic vasculitis and chronic tonsillitis have common antigens - B 27, Cw2, Cw6.
Chronic tonsillitis can lead to eye diseases.
Thus, tonsillogenic intoxication can significantly weaken the accommodative apparatus of the eye. Therefore, an important measure to prevent myopia is early sanitation of the source of chronic infection. Behcet's disease, which causes eye lesions, is also provoked by a focus of chronic streptococcal infection during tonsillitis.
A combination of nonspecific lung diseases and pathology of the palatine tonsils is often noted. Thus, endogenous peribronchitis is provoked by inflammatory processes of the nose, paranasal sinuses and lymphoid pharyngeal ring. Sometimes chronic tonsillitis can contribute to the exacerbation of chronic pneumonia, and also lead to a more severe course of this disease. Pulmonologists note that timely sanitation of a focal infection in the palatine tonsils reduces the number of complications in chronic lung diseases by 2.3 times.
The infectious-toxic mechanism of liver damage in chronic tonsillitis is described. The streptococcal toxin streptolysin O is capable of disrupting the process of oxidative phosphorylation in hepatocyte mitochondria. As a result, existing liver diseases worsen. Thus, with viral hepatitis A, severe and protracted forms are more often observed, and with viral hepatitis B there is a tendency for the process to become chronic. There are known cases of development of damage to the biliary system in chronic tonsillitis.
Cerebral complications in chronic tonsillitis arise as a result of vascular-circulatory disorders and toxic effects from the source of inflammation. The course of cerebrovascular disorders and toxic-infectious encephalopathy occurs in the form of a chronic process or crises. In this case, there are several forms of hypothalamic syndrome. The most common form is the vegetative-vascular form, then the neuroendocrine-metabolic form, and the least common is the neurotrophic form.
A constant and early symptom is cerebral vascular insufficiency due to damage to the cardiovascular system. Hypothalamic angioedema is manifested by a persistent decrease in peripheral blood pressure and signs of peripheral angioneurosis (Raynaud's syndrome). Possible manifestation of cerebral angioedema in the form of migraine or Meniere's syndrome. These paroxysms are superimposed on chronic cerebrovascular insufficiency and are clinically manifested by neurotic conditions. Such “neurasthenia” is accompanied by general weakness and increased fatigue during mental and physical stress. With functional insufficiency of the hypothalamus, patients become sensitive to adverse meteorological factors.
Sometimes neuro-endocrine disorders occur: obesity or weight loss, loss of appetite, thirst, hyperhidrosis, menstrual irregularities, decreased sexual potency. Due to damage to the nuclear stem structures, paroxysms of loss of skeletal muscle tone appear. Smooth muscle tone also decreases. Stem disorders are a consequence of chronic circulatory insufficiency, toxic-infectious and autoallergic processes that occur during chronic tonsillitis. Hypoxia of the respiratory center is manifested by irresistible yawning at the slightest mental or physical fatigue.
It has been proven that women suffer from such disorders more often, since their hypothalamus is subjected to greater physiological stress.
Chronic tonsillitis aggravates the course of schizophrenia. As a result of autointoxication, the disease becomes progradient or malignant.
In the early stages of development of chronic tonsillitis, there is a compensatory increase in the level of androgens and glucocorticoids. As the disease develops, there is a gradual depletion of the function of the adrenal cortex with all the ensuing consequences for the body.
Focal infection in the palatine tonsils can lead to weakening of the islet tissue of the pancreas and the release of a proteolytic enzyme that destroys endogenous and exogenous insulin. As a result, chronic tonsillitis can contribute to the decompensation of carbohydrate metabolism disorders already existing in the body, leading to an increase in hyperglycemia and glycosuria. In turn, metabolic disorders in diabetes form favorable conditions for exacerbations of chronic tonsillitis. Sanitation of the pharyngeal source of infection improves carbohydrate metabolism, which confirms the pathogenetic relationship of these diseases. Some researchers believe that conservative treatment of tonsillitis with this combination is ineffective and a tonsillectomy is necessary after a year. Follow-up data indicate that in patients with diabetes mellitus, surgery contributes to stable compensation, and in some cases allows to reduce the dose of insulin.
With chronic tonsillitis, the thyroid gland suffers. Most often, there is an increase in hormone-forming function.
This disorder is associated with hyperstimulation of the thyroid gland by thyroid-stimulating hormone from the pituitary gland. The consequence of this will be an increase in the concentration of thyroxine in the blood. This process is explained by the effect of pathologically altered palatine tonsils on the hypothalamic-pituitary system. Another possible mechanism for damage to the thyroid gland is associated with disorders of the immune system. Thus, in individuals with a genetically determined predisposition to autoimmune thyroid diseases, diseases such as autoimmune Hashimoto's thyroiditis, subacute de Quervain's thyroiditis, Riedel's fibrous thyroiditis, and acute thyroiditis may occur. It has been noted that the severity of pathological changes in the thyroid gland depends on the duration of chronic tonsillitis and the frequency of its exacerbations. As a result of successful treatment of the pathology of the palatine tonsils, one can observe an improvement in the condition of the thyroid gland and normalization of its hormonal synthetic function.
There is evidence of a high incidence of chronic tonsillitis in obesity, which may be due to damage to the ventromedial and ventrolateral nuclei of the hypothalamus. In the decompensated form of chronic tonsillitis in combination with obesity, there are significant disturbances in the hormonal status (decrease in the level of testosterone and follicle-stimulating hormone and increase in luteonizing hormone). Children with such disorders have clinical signs of delayed sexual development (adiposogenital dystrophy). Chronic tonsillitis aggravates changes in the hypothalamic-pituitary regulation of the testes and delays the onset of puberty.
Modern studies have proven the pathogenetic role of tonsil apudocytes in the development of immunodeficiency states.
In chronic tonsillitis, a threefold increase in cells of the APUD system is recorded, cells producing serotonin and somatostatin appear, and the number of mast cells increases. Such changes may also be one of the reasons for the development of pathological changes in other organs.
It has been proven that chronic tonsillitis has an adverse effect on the formation of the reproductive system in girls.
Exacerbation of chronic tonsillitis and the transition of its compensated to decompensated form are more often observed at the age of 8-10 years (adrenarche period) and 12-14 years (menarche period), i.e. during activation of the endocrine function of the pituitary-adrenal system (adrenarche) and the entire reproductive system (menarche).
Our studies have shown the presence of a direct relationship between chronic tonsillitis, especially its decompensated form, and disorders in the reproductive system in women of fertile age. These changes are characterized by disruption of the production of hormones such as follicle-stimulating, luteinizing, luteotropic, somatotropic, adrenocorticotropic and thyroid-stimulating, the appearance of uterine bleeding, hypomenstrual syndrome and amenorrhea of central origin. Such disorders in patients with chronic tonsillitis can be considered a manifestation of hypothalamic-tonsillar syndrome. Damage to the hypothalamic region is indicated by characteristic changes in the electroencephalogram. Changes in hormonal levels can provoke diseases such as endometriosis, adenomatosis and uterine fibroids.
With chronic tonsillitis, the development of pregnancy pathology is often observed, since it contributes to a significant decrease in the body's adaptive capabilities and is a predisposing factor for the formation of toxicosis. There is often a threat of early or late miscarriage or premature birth. Deviations of labor may develop, such as premature rupture of amniotic fluid, weakness of labor.
Often chronic tonsillitis leads to hypogalactia due to hypothalamic-pituitary disorders.
We believe that patients with combined pathology of the tonsils and reproductive system should be under constant medical supervision by an otolaryngologist and gynecologist.
There is a tendency to normalize hormonal synthetic function and clinical signs of reproductive disorders as a result of successful treatment of chronic tonsillitis.
Most patients with a decompensated form of chronic tonsillitis have abnormalities in the morphogram (intersex physique). A characteristic set of symptoms is disproportionate, inharmonious, asynchronous development. False acceleration syndrome often occurs, which can be considered a variant of sexual infantilism.
All of the above allows us to conclude that patients with chronic tonsillitis form a large risk group for many severe somatic disorders and require increased attention from both an otolaryngologist and doctors of other specialties. Only such an integrated approach can reduce the number of complications in patients with chronic tonsillitis.
Published with permission from the administration of the Russian Medical Journal.