Milk and molar teeth in children
Many people believe that there are no differences between permanent and temporary teeth, but this is not true. So, how to distinguish a baby tooth from a molar? At a minimum, their number differs (milk - 20, permanent, as a rule, 32). Temporary teeth have a light shade, while permanent teeth are naturally more yellow. Indigenous ones are also significantly larger in size than dairy ones - visually it is quite easy to distinguish them. Here are the most common questions asked by Internet users on this topic.
- Do children have molars?
Of course, there are, and at a certain point they begin to actively erupt. - How many molars do children have?
From 28 to 32 (the maximum set appears after all eights appear). - Which molars appear first in a child?
Typically, the lower central incisor erupts first. - At what age do children start to get their molars?
Usually, dentition renewal begins after 6–7 years, but there are no strict limits. - Do children lose molars?
By themselves - no, as a result of injuries and illnesses - yes. - What are the risks of removing a molar tooth in children?
As corny as it may sound, his loss. And yes, a new one will not grow. Everything is like adults. - What to do if a child has yellow molars?
Permanent teeth have a more yellowish tint than temporary teeth. Plaque on a child’s molars is normal, but hygiene should never be neglected. - What to do if a child has black molars?
When teething, baby teeth may have a black color (the so-called Priestley plaque, or pigment bacteria). However, this does not happen with molars. If they are black, go to the dentist immediately. - What to do if a child does not have molar buds?
This happens, but very rarely. Fortunately, with modern implantation and prosthetics technologies, the problem can be solved. - Is it normal for a child to have crooked molars?
Contact an orthodontist immediately: correcting a bite in childhood is much easier and faster than in adults. - Which teeth do children replace with molars?
All twenty, plus new molars appearing.
Second lower premolar
Average age of teething: 11-12 years
Average age of root formation: 13-14 years
Average length: 22.3 mm
The second lower premolar, which is very similar in crown shape to the first premolar, has a less complex root.
Its crown has a well-developed buccal cusp and a much better formed lingual cusp than on the first premolar. The access is made slightly oval, wider in the mesial-distal direction. They begin to form access in the central sulcus with a fissure bur with a cutting apex, and then expand and form the contour of the burr hole with spherical burs No. 4 and 6.
Researchers reported that only 12% of mandibular second premolars studied had a second or third canal [17]. Vertucci [13] also showed that second premolars had one apical foramen in 97.5%, while only 2.5% of the teeth examined had two foramina.
An important circumstance that should not be forgotten is the anatomical location of the mental foramen and the vessels and nerves passing through it. Due to the proximity of these structures, an acute inflammatory process in the area of the lower premolars can cause temporary paresthesia. The exacerbation of the pathological process in this area is more severe and resistant to conservative treatment than in other areas.
Molars in children: symptoms of eruption
- Fever. When teething in children, body temperature may rise, usually not higher than 38 degrees.
- Itching and pain at the site where the molar appears. Various gels and ointments, as well as gum massage, will help relieve children from unpleasant sensations.
- Increased salivation and runny nose.
Important!
The growth of molars in children, especially at the initial stage, leads to weakened immunity. Take vitamins and do not forget about preventive visits to the dentist.
Injuries
An accident or incident, such as a fight, can cause a tooth injury. And it doesn’t matter whether a small part has broken off, or the tooth has cracked, as they say, “to the point of bleeding” - the help of a doctor is definitely needed. In some cases, lost dental tissue is replenished. If a tooth is broken into pieces, it will most likely need to be completely removed and a prosthesis replaced every year. And the answer is simple - the dental tissues have not yet fully matured, the body is growing. And it is necessary to take full care of your teeth at such an early age. In case of extension, the operation is performed by introducing composite materials that replace enamel and dentin.
When does a child's molars come out?
Most parents are interested in the question: at what age do children’s molars begin to erupt? The first buds form in the fifth month of pregnancy. The exact timing of their appearance has not been determined and depends on the individual characteristics of the organism. Nevertheless, an approximate scheme for the eruption of molars in children exists. If the appearance of a permanent tooth is delayed for more than six months from the extreme threshold (especially after the loss of a baby tooth), consult a specialist. The doctor will take control of the process and be able to identify complications.
Possible problems
Despite the fact that changing teeth is a natural physiological process, some children and their parents may encounter a number of problems that require contacting a pediatric dentist.
No molars
The absence of permanent units can be caused by congenital edentia - the complete or partial absence of tooth buds.
Another reason for the absence of molars is previous inflammatory diseases - periostitis or periodontitis, resulting from progressive caries. Inflammatory diseases of the periosteum and periodontal tissues have an extremely negative effect on the condition of the tooth buds and can lead to their death.
Important! It is absolutely necessary to treat baby teeth for caries. You should not assume that the problem will go away on its own with the change of teeth. The progression of the disease can negatively affect the health of the tooth buds.
Molar tooth hurts
The enamel of newly emerging permanent teeth is still poorly formed. The low level of its mineralization makes teeth vulnerable to cariogenic microflora. This can lead to the development of caries and cause pain.
Due to poorly formed enamel, tooth sensitivity to external irritants (cold, hot, sour, sweet) may increase, which is also accompanied by painful sensations.
Important! Normally, permanent teeth do not hurt. If pain occurs, you should contact your pediatric dentist. The specialist will determine the cause of the pain, carry out the necessary treatment, fluoridation or remineralization of tooth enamel.
Molars grow crooked
The incorrect position of permanent teeth can be caused by two reasons - the growth of the permanent unit outpaces the process of loss of baby teeth or they were removed ahead of schedule, which led to incorrect formation of the rudiments of permanent teeth.
In this case, there is only one way out - orthodontic treatment of malocclusion.
Important! A malocclusion must be corrected. The sooner you contact a dentist, the more successful the treatment will be. The child will be prescribed to wear removable or fixed orthodontic appliances that will help straighten the permanent teeth and bite.
Injuries
Due to their activity and lack of experience, children can accidentally injure a newly emerging permanent tooth. Due to mechanical damage, cracks and chips may appear on it. The damage looks unattractive. Caring for such teeth is complicated, since food debris can get stuck in the cracks, which will certainly lead to the development of caries.
Important! If a child accidentally injures a permanent tooth, it is necessary to seek help from a dentist. The specialist will assess the complexity and depth of the damage and will build up the missing volume of tooth tissue with composite materials.
Tooth loss
Loss of healthy permanent teeth can only occur as a result of severe trauma to the jaw, for example, during a child’s fall or fight. A diseased molar may fall out on its own. In this case, you will also need to consult a specialist. Most likely, the child will undergo temporary prosthetics for the lost unit, which will not disrupt the formation of a correct permanent bite.
The tooth is loose
Looseness of a permanent tooth is an alarming symptom indicating a pathology of the dentofacial apparatus or the presence of inflammation. Consultation with a specialist is required!
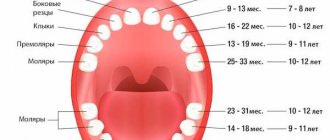
Pattern of growth of molars in children
In most cases, the permanent tooth appears 3 to 5 months after the temporary tooth falls out. The order of eruption of molars is in many ways similar to the appearance of milk teeth. The first molars in children are the central lower incisors. The upper permanent teeth develop later than the lower ones, if we consider them in pairs.
| Age | Eruption of molars in children |
2 years | There have been references in history where a child was born with one or more molars. Cases when molars erupted in a 2-3 year old child also occur, but are extremely rare (less than 1%). |
5 years | When a child is 5 years old, molars very rarely come out (less than 10% of the total). If a baby tooth falls out on its own at such an early age, then there is every reason to believe that a permanent one will soon appear in its place. |
6 years | The roots of baby teeth (especially the upper and lower incisors) begin to dissolve and the teeth fall out. Usually, it is at the age of 6 that a child’s first molar begins to erupt. |
7 years | At this age, the first lower molars in children (at least one of them) have already erupted and the incisors of the upper jaw are next in line. |
9 years | At the age of 9, a child’s second molar should definitely have time to appear. Some children acquire lateral incisors and even a premolar on one of the jaws. |
10 years | At the age of ten, children’s back molars begin to actively erupt (premolars, and a little later – molars and canines). |
13 years | At 12–13 years of age, children usually develop a full bite of permanent teeth. The last teeth to emerge are usually the upper canines and second molars. This does not apply to wisdom teeth, which appear in adulthood (after 17–18 years) or may not erupt at all. |
Location and anatomical features of molars
Since man is an omnivore, for a healthy metabolism he needs different foods, including rough, animal, and plant foods. In order for the body to absorb it, you need to chew the food well, which is what molars do. Their chewing area reaches 1 cm2. Each such organ can withstand pressure of up to 70-75 kilograms. In total, there are up to 12 such units in the oral cavity of an adult. Six of them are located on the lower jaw, six on the upper jaw, three on each side.
The last elements in the series are the third molars. They are also called wisdom teeth. They cut through in adults, and often may not cut through at all. Their roots can have two, three or more branches. The size of the crowns of molar units can reach from 7 millimeters, in some organs up to nine. Their chewing surface is diamond-shaped with rounded corners. It has four tubercles, which are separated by 3 grooves located transversely. Classification of roots:
- palatal;
- buccal-distal;
- buccal-mesial;
The last type of roots is the largest. The palatine root belongs to the middle ones. The shortest in size is the buccal-distal. Each subsequent molar unit is endowed with smaller roots and a crown portion than the previous one. The first molar organs are large, their coronal surface is significant in area, and the size of the roots is the largest. The second units are already smaller in size. The extreme units do not have milk precursors. Their root length and crown size vary significantly. Usually, there are 3 tubercles on the crown, one of which is lingual and 2 buccal. As a rule, their roots are not too long, but they are often displaced and deviated to the side. Wise teeth can come into contact with 2 antagonists at the same time. This is considered normal.
On the upper jaw
The top row has its own characteristics and differences. Their main aspect is location. They form a straight line that is only slightly curved and diverges to the sides. The slope of the units increases from the first to the third segment. In addition, in the upper teeth:
- Larger in size than the organs located in the lower jaw;
- The root system is more powerful, it has three roots;
- The tooth surface area is extensive;
- Good ability to chop and chew food;
- The outer side is covered with sharp tubercles with protruding forms, there are 3 or more of them;
The second molars of the upper row in the coronal part are similar to the first molar units, although they are more massive and rectangular. They are easier to dissect. The roots are usually grouped, sometimes merging with each other. The canals, which are parallel, often overlap each other when X-rays are taken. The roots are shorter compared to previous teeth. The three mouths often form a flat triangle, less often a straight line. The convex bottom of the chamber gives the mouths a funnel shape. It happens that the channels to the bottom of the chamber bend at a very acute angle.
Rarely do the upper posterior units have four roots. The first molar large organ of the upper jaw is equipped with more powerful roots than its lower antagonist. The peculiarity of the second molar teeth is that their crown can have any shape, while the lower ones can only have a certain shape. Properties of the shape of the upper units: cubic, regular, with a clear cross-shaped groove that divides the surface into four parts. The eights that are located on top are smaller in size than the bottom ones. In addition, they can develop from 1 to 4 or more roots.
On the lower jaw
Molars on the chewing side have tubercles, as well as fissures, that is, grooves. They can be shaped like cones, drops, or grooves. Reliefs are formed during the formation of organ rudiments. Since they grind food, there is a high risk of caries. To avoid such a pathology, it is necessary to seal the fissures. The procedure prevents food particles from getting into the grooves. In addition, sealants nourish the enamel layer with fluoride, helping it become healthier. To achieve maximum effectiveness, the session is carried out immediately when the units erupt, or within 12 months.
The molar organs of the lower row differ from the segments of the upper jaw. Their features:
- Such units have a different anatomical structure.
- They most often have 3 canals and 2 roots.
- They are smaller in size than their antagonists.
- The number of tubercles varies from three to six.
- The distal and medial roots are parallel.
- Root fusion is often diagnosed.
- The crown of the first unit has the shape of a cube, it is slightly elongated in the direction of the dentition.
- The most posterior wise crowns are always large in size, they are larger than the upper ones.
- As a rule, they have two roots that can grow together into one.
- The fissure tubercles are lower, blunt, and have a rounded shape.
The bottom row is located almost in a straight line. The crowns are inclined in the opposite direction than on the upper segment. Because of this, when the jaw bones are closed, the upper row is superimposed on the units of the lower jaw with a slight shift outward. The crowns of the 2nd molar tooth are slightly smaller than the coronal part of the first unit. The approximal surfaces are located almost parallel. They taper slightly at the neck. The vestibular surface is divided into 2 parts by a rather deep notch.
Complications during teething
- Delay in the appearance of permanent teeth.
This may be due to genetic characteristics, immune system problems and a number of other diseases. - Uneven teeth and other malocclusions.
- Hyperdentia.
The child’s molar tooth (or teeth) grows in the second row. Hyperdentia, or supernumerary of teeth, is a fairly rare phenomenon, but requires the intervention of a dentist to eliminate the risk of malocclusion in a child.
What does the dental formula look like?
The medical record, which the big one keeps in the dental clinic at his place of residence, contains notes about his dental condition. To avoid confusion, doctors number the teeth on each side of each jaw. So, the 1st and 2nd teeth are incisors, the 3rd are canines, the 4th and 5th are small molars (doctors call molars molars), the 6th and 7th are large molars. The 8th - the farthest one - is a “wisdom tooth”; a number of people do not have it, or they do, but not all. Each side of the jaw is also numbered: 1 - top right, 2 - top left, 3 - bottom left, 4 - bottom right. For example, entry 48 does not mean that you are a “Tarkatan” with a combat superset of teeth that does not exist. You simply do not have a “wisdom tooth” on the lower right. Entry 41 - a person lost one of the frontal incisors on the same side on the same jaw. You can write down the formula of the teeth more clearly: for example, “there is no 8th tooth from the bottom right.”
It often turns out that due to lack of space on the jaw, the wisdom tooth develops incorrectly - it can grow crooked, in which case its removal is indicated. For example, it may remain under the gum and, because of this, be affected by caries, which can subsequently develop into pulpitis or a dental cyst. Problematic “wisdom teeth” are quickly and decisively removed, and their absence will not greatly affect the quality of chewing food.
Common problems with molars in children
| Problems with molars | How to fix? |
| Molar tooth is loose | A common occurrence with injuries and bruises. To avoid tooth loss, an urgent visit to the dentist and the application of a special splint are necessary, especially if the child’s molar sways when touched. |
| Broken molar tooth | Severe chips may require orthopedic treatment. If a child's front molar has chipped, aesthetic restoration with veneers or crowns may be required. |
| Molar caries | When the first molars erupt, it is important to prevent the occurrence of caries. If this happens, then it is necessary to stop the disease in its infancy, otherwise it will affect the deeper layers of the tooth. |
| A child's molar has fallen out | The most unpleasant thing that can happen. If a child knocks out a molar along with the root, then there is a chance to save it. To do this, you need to place the knocked out tooth back into the oral cavity, saline solution or into a glass of milk and urgently rush to the dentist (you need to do it within 30 - 40 minutes after the injury). If a child’s molar tooth has been removed, then there is only one way out - installing a prosthesis. |
Anatomy of permanent teeth
The molar tooth includes three zones: the root, which sits deep in the jaw socket and holds the tooth in place, the neck, located in the periodontal area, and the crown, which extends directly into the oral cavity. After the apex of the tooth appears, a protective film forms on the enamel, the strongest layer of the tooth, which is soon replaced by a salivary layer, formed from the saliva itself. The dental tissues themselves are not just a piece of bone, but a certain heterogeneity, which includes, in addition to enamel, dentin (the main substance of the tooth) and the dental cavity, in which nerves and blood vessels branch. Compared to bones, for example, the phalanges of the fingers, dentin is noticeably stronger - it contains an increased amount of minerals, for example, the same calcium-based compounds. The root zone of dentin is connected to the periodontium using a special layer - dental cement, which communicates with the tissues of the periodontium itself and supplies the dentin with nutrients.
Care instructions
Molars in children require even more careful care than in adults. Frail enamel is much more susceptible to the effects of carious bacteria and the external environment, and the love of sweets and carbonated drinks does not add strength to it. When children develop a permanent bite, parents need to take special control of oral hygiene and diet (at least until the age of 14–15, when the teenager himself begins to realize the importance of dental health). In general, there are no difficulties here: in order to keep children's teeth strong and healthy, you need to follow several basic points.
- Daily hygiene.
Brush your teeth at least twice a day, use dental floss and special rinses. - Proper diet.
Limit your intake of sweets and carbohydrates. - Preventative visits to the dentist at least once every six months.
If necessary, fluoridation and sealing of molars in children (so-called fissure sealing). - Do not forget to wear a protective mouth guard during active games and sports.
Is there always a change?
Not a single child's tooth should be preserved - they all fall out. Instead of each temporary one, a permanent one is cut through. But it also occurs in dental practice that the rudiment of the root unit is missing. This can be seen in the X-ray of the jaws.
In this case, the life of the baby tooth is extended to the maximum - after all, nothing will grow in its place. When an empty space appears in the dentition, the issue of prosthetics is discussed.
To eliminate partial congenital edentia, you can implant an implant or install a dental bridge. In the first case, there is no need to file adjacent teeth. The doctor, under local anesthesia, installs an artificial titanium root into the jaw tissue. When it takes root, it fixes the dental crown.
In the case of a bridge, it is necessary to depulpate and prepare the neighbors . This is not very healthy, since their service life after such manipulations is significantly reduced. Therefore, young patients who do not have separate molars are recommended by dentists to resort to implantation.